new technique for pain management ,described by dr forero ,it can replace epidural anesthesia,paravertebral anesthesia and other regional blocks.it can be used for both acute and chronic painful conditions
new technique for pain management ,described by dr forero ,it can replace epidural anesthesia,paravertebral anesthesia and other regional blocks.it can be used for both acute and chronic painful conditions
Erector spinae plane block is a relatively novel approach to pain management for a variety of surgical procedures. ESP block is a challenging anesthesia and analgesia technique that needs more research.
The transversus abdominis plane, more commonly referred to as the TAP block,
Places local anesthetic in the lateral abdominal wall in a plane between the internal oblique and the transversus abdominis muscles.
Here, the local anesthetic block can block many of the abdominal nerves as they pass to the abdominal structures.
Anesthetic consideration in smokers,alcoholics and addictsAftab Hussain
Anaesthetic consideration in smokers alcoholic and drug addicts. As an anaesthesiologist we must be aware with the problems associated with their management and interaction with anaesthetics.
Neuromuscular monitoring, also known as train of four monitoring, is a technique used during recovery from the application of general anesthesia to objectively determine how well a patient's muscles are able to function. It involves the application of electrical stimulation to nerves and recording of muscle response using, for example, an acceleromyograph. Neuromuscular monitoring is typically used when neuromuscular-blocking drugs have been part of the general anesthesia and the doctor wishes to avoid postoperative residual curarization (PORC) in the patient, that is, the residual paralysis of muscles stemming from these drugs.
Erector spinae plane block is a relatively novel approach to pain management for a variety of surgical procedures. ESP block is a challenging anesthesia and analgesia technique that needs more research.
The transversus abdominis plane, more commonly referred to as the TAP block,
Places local anesthetic in the lateral abdominal wall in a plane between the internal oblique and the transversus abdominis muscles.
Here, the local anesthetic block can block many of the abdominal nerves as they pass to the abdominal structures.
Anesthetic consideration in smokers,alcoholics and addictsAftab Hussain
Anaesthetic consideration in smokers alcoholic and drug addicts. As an anaesthesiologist we must be aware with the problems associated with their management and interaction with anaesthetics.
Neuromuscular monitoring, also known as train of four monitoring, is a technique used during recovery from the application of general anesthesia to objectively determine how well a patient's muscles are able to function. It involves the application of electrical stimulation to nerves and recording of muscle response using, for example, an acceleromyograph. Neuromuscular monitoring is typically used when neuromuscular-blocking drugs have been part of the general anesthesia and the doctor wishes to avoid postoperative residual curarization (PORC) in the patient, that is, the residual paralysis of muscles stemming from these drugs.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Anti ulcer drugs and their Advance pharmacology ||
Anti-ulcer drugs are medications used to prevent and treat ulcers in the stomach and upper part of the small intestine (duodenal ulcers). These ulcers are often caused by an imbalance between stomach acid and the mucosal lining, which protects the stomach lining.
||Scope: Overview of various classes of anti-ulcer drugs, their mechanisms of action, indications, side effects, and clinical considerations.
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
1. Guide- Dr MADHEKAR MA’AM
STUDENT- DR ASHISH NAIR
AANA journal/August2007/Vol.75,No.4(277-85)
ATOTW 397 — Introduction to Intraoperative Neurophysiological
Monitoring for Anaesthetists (5 February 2019) Page 1 of 11
2.
3. OVERVIEW
Anatomy and definition
History
Types
Prevalence
Signs & symptoms
Severity and Cobb’s angle
Effects of kyphoscoliosis on various organ systems
Surgical correction
Preoperative evaluation
Management of anaesthesia
4. DEFINITION
• Kyphoscoliosis describes anabnormal curvature of thespine
inboth coronal andsagittal plane
• Kyphosis is acurving of thespine thatcauses a bowing of
the back
• Scoliosis is definedasalateralrotation of the spine greater
than10 degrees accompanied by vertebral rotation
Scoliosis involves:
I. lateral curvature of spine
II. Vertebral body rotation
III. Angulation of the ribs leading to thoracic rib cage
deformity
5. HISTORY
5th century – HIPPOCRATES described
Galen(AD 131-201) termed scoliosis
Galen also used chest binders to aid spinal curvature
Pare (1510-1590) developed iron corsets
Jules Guerin(1839)- first surgical Rx
Sayre(1880s)-POP in vertical suspension device
Lange(1902)-spinal fusions in TB kyphosis
Hibbs(1914)- spinal fusion for scoliosis
Harrington(1955)-distraction rods for Rx of scoliosis in
polio
Luque(1970s)-used Harrington or Luque rods for spine
fixation(now currently used) aka Cotrel-Dubousset rods
8. 3.CONGENITAL
SCOLIOSIS(with/without neuro
deficit)
Open,with posterior spinal defect
Closed,no posterior element defect
i. -Abnormality of development of vertebrae –
hemivertebrae/congenitally fused ribs
ii. -½ cases associated with other organ system abnormalities
4.Neurofibromatosis
5.Mesenchymal disorders
congenital-Marfan’s syndrome, morquio syndrome,Ehlers Danlos
syndrome
Acquired- rheumatoid arthiritis, still disease
Others-osteogensis imperfecta
5.Trauma
Vertebral-fracture,surgery, Post radiation
Extravertebral-Post thoracoplasty, burn
9. Mc form is- adolescent idiopathic scoliosis(AIS)
Children between age of 10-16 yrs
PREVALENCE
• Curves >10° :1.5 – 3% ofpopulation
• Curves >20° :0.3 to 0.5%
• Curves >30° :0.2 to 0.3%
• Most curves convex to the right
• Males are more likelyto have infantile/juvenile
scoliosis
•Females-adolescent scoliosis
12. TYPESOF KYPHOSIS
• Postural kyphosis
– most common type
• Scheuermann's kyphosis
– aform of juvenileosteochondrosis of the spine
• Congenital kyphosis
• Nutritional kyphosis
– Vit D deficiency
• Gibbus deformity
– Tuberculosis
• Post-traumatic kyphosis
14. ADOLESCENT IDIOPATHIC SCOLIOSIS
Mc deformity of spine
Near onset of puberty
Lateral curvature and vertebral rotation of more than 10
degree
1-3%incidence in adolescents(10-16yrs)
Females more affected than males
Ratio 3.6 to 1
spinal bracing can slow progression and prvent need for
surgery
4 curve patterns –thoracic,lumbar,thoracolumbar,double
major curves
15. SIGNSANDSYMPTOMS
• Back pain
• Leg length discrepancy
• Abnormal gait
• Uneven hips or waist
• One shoulder higher than other
• Prominent shoulder blade.
• Appearance of leaning to one side
• Increased space between the body and
the elbow while standing in natural
posture.
• Chest/rib prominence.
18. ASSESSMENT OF SEVERITY
Cobb’ s angle(1948)
• Tomeasure coronal plane
deformity on antero-posterior
planeradiographs in the
classificationof scoliosis
• Determining severity of
disease
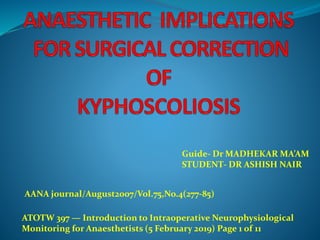
19. MEASUREMENTOFTHECURVE INSCOLIOSIS USINGCOBB'S ANGLE
• Identify the
upper and lower
end vertebrae
• Draw lines
extending along the
vertebral borders.
•Measure the cobb
angle(5)
The cobb angle is derived from the angle between intersecting lines drawn
perpendicular to the top of the uppermost affected vertebra and the bottom of
the lowermost affected vertebra.
20. The degree of spinal curvature at skeletal maturity aids
in predicting the magnitude of curve progression for
the lifetime of the patient
Weinstein et al
<30 deg- minimal disease progression
>30 deg – progression of 19 deg in life span
>50 deg – 1-2 deg progression per year
Surgery is indicated @ 40-50 degree
“Double curve patterns of the thoracic and lumbar
spine are more likely to progress than single curve
patterns “
“Larger curves have greater risk of progression”
21. COBB’ S ANGLE
Greaternumberofvertebrae involved
More cephaladlocationof curve
Loss ofnormalthoracic kyphosis
Neuromusculartypes
Scoliosisseverityincreases with:-
23. • Stand erect with feettogether &knees fullyextended & palms
touching each other
• Bending forward until back is horizontal
• Asymmetry of thoracic or lumbar spine maybe detected with
Scoliometer
• Measure Angle of Trunk Rotation(ATR) atthoracic,thoraco
lumbar &lumbar areas of spine
ADAMS FORWARDBENDTEST
24. TREATMENT
• Surgical intervention occurs when the curve magnitude estimated by the
Cobb methodis morethan40 degrees
• Fusevertebraeinamore normalcurve
• Severecurves:leadingto cardio-respiratory compromise
• AIM :to achievespinalfusionincorrected position
– Decortication &maintainingcorrection till bonyfusionwith
thehelpof instrumentation
• Erector spinae,spinousprocess,intraspinal ligament,facetjoint
removed
• Vertebraedecorticated&bonegraft placed
25. Flexible thoracic curve(without lumbar curvatures)-
posterior spinal fusion with instrumentation
Stiff thoracic curve-anterior approach is required
- gains spinal mobility
- improve posterior correction
Thoracolumbar curves- more challenging
- increased manipulation
- increased surgical time
- increased blood loss
- increased risk of neuro. complications
28. RESPIRATORY SYSTEM
Cobb’s angle >50 deg at skeletal maturity
Reduces the mechanical efficiency of the chest wall- restrictive
lung disease
• Restrictive pattern is seen- ↓↓vital capacity(60-80% of
predicted)
• As the thoracic curvature increases- VC(max),FEV1,PaO2 ↓
↓TLC,↓FRC,↓IC,↓ERV.
↓IC with normal expiratory flow results in diminished FEV1 and
FVC but the FEV1/FVC ratio remain normal
• During exercise the ventilation is adequate but there is ↓TV and
↑RR the maximum work capacity decreases.
• Cobb’s angle 70-100 deg -> severely restrictedventilation
->alveolar hypoventilation ->AV shunting -> cor pulmonale
29. A preoperative vital capacity of less than 35% is considered a
relative contraindication for surgery.
“thepresence of an adequatecoughis agoodclinical indicator of a
satisfactoryforcedexpiratoryvolume.”
PFT
pulmonary function is most closely related
- to Cobb angle
-number of vertebra involved in the scoliosis curve
-location of the upper-most vertebra
-patient age
CauseofabnormalPFT
• Due to abnormalthoraciccagegeometryleadingto marked
decreaseinchestwall compliance
thelungsandrespiratorymusclesarenormal exceptin
congenitalandinfantiletypewherethe growth ofthelungsmay
be impaired.
30. BLOOD GAS ABNORMALITYIN SCOLIOSIS
• Arterial hypoxemiaismainlybecauseofventilationperfusion
mismatch.(ArterialO2 desaturation)
• pCO2 andpH arenormal(initially)
↓ diffusingcapacityandalveolarhypoventilationmay contribute.
• Severelongstandingscoliosis isa/wmarkedV/Q mismatch,
alveolarhypoventilationandCO2 retention.(hypoxemia,hypercapnia,
secondaryelectrolyteabberations)
• ifnot surgically treatedmayleadto PAH and respiratory failure.
•Symptoms of upper and/or lower respiratory infection should prompt a
thorough examination.
•Anesthetists and surgeons may want to consider postponing the surgery
for 4 to 6 weeks to allow full recovery from th e respiratory infection.
31. Cardiovascular system
• Maybeassociatedwith↑pulmonaryvascularresistanceand
pulmonary hypertension.
•MayresultinRVH andRightventricular failure.
•Cause- hypoxemia→pulmonaryvasoconstriction → ↑PVR →
↑PA pressure.
•Chronic hypoxemia→PAH.
•Hypoxic pulmonary vasoconstriction takes place in the face of
reduced PaO2
• A/wwithmitralvalveprolapse.Antibioticprophylaxisbefore
catheterization&laryngoscopy
Cardiomyopathy-Duchenne’smuscular dystrophy
Mitral/aortic insufficiency-Marfan’s syndrome
Congenital heartdiseaseis common.
34. Physical examination
o Auscultation of lungs for anywheeze(obstructive or
parenchymallung disease)
o Heart-signs of PAH(loud P2)and signs of
RVH(engorged veins,hepatomegaly,edema)
oSkin-caféaulaitspots in NF
• Airway assessment –
I. to see for cervical scoliosis
II. high arched palate(Marfan’s)
III. neurofibroma.
o Neurological assessment- pt with pre existing neurological deficit
areat↑risk of spinalcord injury during surgery .
o Also documentation of pre op neurological statusis imp.
35. EXERCISE TOLERANCE
Maximal Oxygen Consumption (Vo₂ Max) : Most useful
predictor of post thoracotomy outcome
Vo2 max= 15 (HRmax/HRrest)
-Vo₂ Max > 15ml/kg/min – tolerate pneumonectomy
-Vo₂ Max 10-15ml/kg/min - High risk and requires
careful evaluation
-Vo₂ Max < 10ml/kg/min- inoperable
Traditional : Stair Climbing
5 Flights = Vo₂ Max > 20ml/kg/min
(1-flight== 20 steps– 1 step 6 inchs)
SHUTTLE WALK TEST- b/w 2 points 10mts apart (inc. speed
every minute)
6 MINUTE WALK TEST
-walk on level ground at max pace
-< 2000 ft = Vo₂ Max < 15ml/kg/min
36. INVESTIGATIONS
•Haemogram
•O2 carrying capacity
•Guide to transfusion
•RFT,LFT,Coagulation studies
•Chest radiograph(cxr)
•Ecg(document caridac ischemia and axis deviation)
•2D echo(cardiac function and rule out sturctural abnormality)
•ABG :Hypoxemia
•V/Q abn.> alveolarhypoventilation
37.
38. •Pulmonary function tests
•Spirometry(extent of restrictive lung disease)
•FVC
•FEV1/FVC
•PEFR
•Peakinspiratory pressure
•Peakexpiratory pressure
•Vital capacity< 40% normal
•Req of postoperative ventilation
•CC > FRC
•Decreased DLCO
39. ANAESTHETIC TECHNIQUE
• PriortoOT psychologicalpreparationisamust
-parentcounselling
-counsellingreagardinwakeuptest
-Preoperativesedation
• Depends on whether wakeup test is to be used
• NGTas postop ileus is common
• Induction :thiopentone/ propofol
• Maintainence:
-o2+N2O+lowiso+fent+vec
-high dose fentanyl+ TIVA with propofol infusion+ very low/no
isoflurane
• ScH:avoidinmuscle disorders
• P/O painrelief:spinal,epidural,caudal
40.
41.
42. Monitoring &lines
• Twowidebore iv lines
• Standard monitoring :
• ECG,NIBP,SpO2, vapour pressure, EtCO2,Airwaypressures
• Invasiveblood pressure,
• CVP monitoring/ pulm artery catheter if PAH
• Urine output,temperature
• Warm fluids,warmblanket
• Eyecare,pressure points &positioning
• Esophagealstethoscope
•OESOPHAGEAL DOPPLER-CO monitoring
as 20-30% dec in co in prone position
Compression stockings and pneumatic boots and avopid
anticoagulants for DVT prophylaxis
43. INTRAOPERATIVE CONCERNS
• Long duration of surgery
• Difficult airway
• Prone position complications
Blood loss &replacement
• Hypothermia
• Lung isolation
• Spinalcord monitoring (Wake up test &evoked potentials)
• Venous air embolism
Risk of malignant hyperthermia
45. Foam bolsters are commonly used,
o one at the level of the chest below the axillae
o the other at the level of the anterior superior iliac spines.
The arms should be abducted to no more than 90deg with
slight internal rotation and lie in front of the plane of the
body to reducethe risk of brachial plexus injury
the ulnar nerve at the elbow which is at risk of pressure-
related injury when the arms are flexed in the prone
position
If the arms remain by the patient’s side, then the thumbs
should be positioned pointing down to avoid over
pronation
Avoid pressure on the abdomen
46. Prone position &concerns
Arms are abducted less than90 degrees whenever
possible(prone “superman”position)
Pressure points are padded
Soft headpillow has cut outs for eyes and nose and a slot to
permit endotracheal tube exit
Chest and abdomen are supported awayfrom the bed
◦ minimize abdominal pressure and preserve pulmonary
compliance
Eyes checked frequently
Elastic stockings and activecompression devices> lower
extremities >minimize pooling of the blood
47. Montral mattress
Jackson table
Wilson frame
Andrews table
The radius of curvature of
the Wilson frame can be altered by
means of a winding mechanism.
This allows a reduction in the
lumbar lordosis thus improving
posterior surgical access
50. Prone position
Horseshoe shaped
adapter
Superior access to airway &
visualization of eyes
the Mayfield head fixator- The head is held
in a clamp by pins which are inserted into
the outer table of the skull.
51. COMPLICATIONS
the incidence of ischaemic optic neuropathy may be increased compared with other prone-
positioning devices.
52. BLOOD LOSS &REPLACEMENT
• Usually associated with largeblood losses
– 15 to 20 ml/kg
– Typical blood loss for these procedures may exceed 50% of
patient’sblood volume and is directly related to
• Factors
– surgicaltechnique
– operativetime
– numberofvertebrallevels fused
– Whether bone graft is taken from the hip
– increased intra-abdominal pressure
– intermittent positive-pressure ventilation
– Anaesthetics
– meanarterialblood pressureor venous pressure
– plateletabnormalities
– dilutionalcoagulopathy
– primary fibrinolysis
54. BLOOD LOSS
• Techniques to reduce loss
– Avoid light anaesthesia,hypertension, hyperdynamic circulation,
hypercapnia
– Surgical hemostasis &vasoconstrictor use
– Proper positioning – avoid raised intraabdominal pressure
– Deliberate controlled hypotensive anaesthesia
– Pharmacological agents
55. Preoperative autologous blood
donation
Hb> 11g%, HCT> 33%
Not Preferred in smaller children and those with
neuromuscular dis.
Donate 10-15% of blood volume
Collected every 4-7 days starting 2 weeks prior
Last donation no less than72 hours before surgery
Started 1 month before
Oral Fe/Erythropoietin supplementation(400U/kg 4 weeks prior)
56. ACUTE NORMOVOLEMIC HEMODILUTION
Removal of whole blood shortly before anticipated
significantblood loss
If Hb>10gm%(target- Hb-7gm%)
Collected in standard blood bags with anticoagulation
Simultaneous infusion of crystalloid(3:1) or colloid(1:1)
Stored atroom temperature
Re infused during surgery after major blood loss has
occurred
Re infused in reverse order of collection
57. “an infusion of 5% albumin to maintain
CVP(range in study 5-23 mm Hg)
PAWP(range in study 7-27mm Hg).”
“adequate oxygen delivery there is an absence of lactic
acidosis, MAP is 60 mmHg or more, the CI is 2.2
L/min/m 2 or more, and the mixed venous oxygen
saturation is 60% or more.”
“hemodilution was done by removing venous blood
and replacing it with an infusion of crystalloid at a
ratio of 3 mL of crystalloid to 1 mL of blood with a
desired post-hemodilution hematocrit value of
30%.The venous blood is then returned to the patient
at the end of the surgical procedure.”
58. Blood salvage
Blood lost during surgery is collected using
commercially availableequipment and is then
anticoagulated,filtered for clots and debris, centrifuged,
resuspended in saline and reinfused to the patient.
Clotting factors need to be replaced using fresh
frozen plasma.
The technique is unsuitable in the presence of
malignancy or infection.
59. DELIBERATECONTROLLEDHYPOTENSIVE ANAESTHESIA
• Younghealthypatient- meanarterialpressure of50 to 60 mm
Hg(but maintain spinal cord perfusion)
• Adult patientwithcardiovasculardisease:higher
pressures
• scoliosis procedures involve mainly venous
bleeding(valveless epidural veins)
• Pre requisites:invasiveBP &urine output,ABG
• MAP of 50-60mmHg can be achieved with remifenatnil inf
and inhal agent alone without use of vasodilators
60. TECHNIQUES:
highdose inhalational agent
vasodilators: Nanitroprusside, nitroglycerine
-SNP dec. peripheral vascular resistance and BP while
inc. CO and tissue perfusion in the presence of
normovolemia or hypervolemia
- A reflex tachycardia may also occur
B adrenergicblockers: esmolol,labetalol
-controlheartrateanddecreasecardiacoutput,reducing
bloodloss
ᾳ2 agonist:dexmedetomidine
*concern- ↓SC blood flow ↑ chanceof SCinjury
during induced hypotension , overadministration of fluid
and blood to replace surgical losses should be avoided
until after instrumentation is complete.
61. Pharmacological agents
APROTININ
Bovine derived polypeptide(anaphylaxis)
Test dose before prone and not used in next 6months
Reduces blood loss in spine surgeries
Inhibits plasmin &kallikrein and preserves platelet function.
1-2 million KIU bolus - 0.25-0.5 million KIU/hr
Or start @ 4mg/kg LD f/b infusion of 1mg/kg MD
DESMOPRESSIN
TRANEXAMICACID10mg/kg infusion @ 1mg/kg/hr
62. Three main arteries traverse the length of the cord,
including
-1 anterior spinal artery
-2 posterior spinal arteries.
Each arises from the vertebral arteries.
Spinal arteries in the cervical and upper thoracic cord are
also supplied by radicular branches of vertebral ascending
cervical and superior intercostals arteries,
Spinal arteries found in the thoracolumbar cord are
supplied by the artery of Adamkiewicz
arteries of the mid thoracic cord are supplied by
intercostals radicular arteries
cauda equina are supplied by the lower lumbar,
iliolumbar, and lateral sacral radicular arteries.
63. SPINALCORD MONITORING
Postoperative neurologic deficitis one of the most feared
complications
Increased risk in non idiopathic scoliosis
Severe rigid deformity> 120°
Congenital scoliosis
◦ Lipomas, tethered cord, cysts,teratomas
CAUSES OFNEUROLOGICAL INJURY
Direct injurydueto instruments
Spinalcord distraction
Hypotension
Ischemic(loss ofblood supply)
64.
65. SPINALCORD MONITORING
WAKE UPTEST
◦ Oldest and Gold standard
SOMATOSENSORY EVOKEDPOTENTIALS(SSEPS)
◦ Allowscontinuousassessmentofdorsal/ascendingcolumns
MOTOR EVOKEDPOTENTIALS(MEPS)
Monitorstheischemiasensitive ventralgraymatterofthe
descending/anteriorcolumns
ELECTROMYOGRAMS
◦ Integrityofanteriormotor spinal cord
66. WAKE UPTEST
By spine surgeon Pierre Stagnara in 1973
Anaesthetist -Mme Vauzelle
Explainingprocedureprior to surgery
Repeat/enactbefore induction
Stop propofol and MR(30-45mins before)
Switchoffinhalation(20minsprior)
Maintainon opioid
Noreversalneedeif3twitchesarepresentonTOF
PROCEDURE
Firstaskedto griphand,bysqueezinganaesthetistshands.
thenmove legandfeet(bothmovingmeansscrewsarePlacedcorrectly)
Preparationto restrainanyunwanted movement(1-2assistantsneeded)
Ifptmoveshandsbutnotfeet–reducetheamountofdistractionandrepeattest(screwsneed
realignment)
Onceptmovesfeet–deepentheplane
67. Hazards & disadvantages
o assessment of voluntary motor function only provides a
brief assessment of the patient’s condition
o may fail to detect the onset of injury, ischemia, or
nerve injury.
◦ Results influencedby anaesthetics and the cognitive integrity
of the patient
◦ inadvertent extubation of the patientduring movement
in the prone position
◦ air embolism during adeepinspiration
◦ dislodgment of the instrumentation during violent
movements
◦ Injury
68. SSEP
Mostwidely usedmodality
assessonlytheintegrity oftheascending sensory tractsof thedorsal
column.
◦ Allowscontinuousassessmentofdorsal /ascending columns
Monitoring SSEPs does not provide information about the
spinal motor pathways th at can be damaged during
corrective surgery
Stimulation of peripheral nerve
◦ Posterior tibial /mediannerve
The SSEPwaveforms are measured in amplitude and latency.
Amplitude signifies the evoked potential wave ’s peak -to- peak
voltage difference.
Latency represents the time from stimulus to peak of
response.p or cervical/thoracic epidural electrodes
69. PN
Dorsal column of
spinal cord
Ascends the dorsal
column
Medulla
Crossess the midline
Contralateral thalamus
Primary somatosensory
cortex
70.
71. The electrical activity is recorded via scalp electrodes
Increased latency>10-15% significant
decreased amplitude >50 % significant
Muscle activity disturbance eliminated by NMB
Affected by hypotension, hypothermia,hypocarbia,
hypoxemia, anemia,andanesthetics
73. MEP
Assess the integrity of the descending spinal motor
pathways (anterior and lateral corticospinal tracts
columns )
Electric or magnetic trans-cranial stimulation
Epidural ,neurogenic or myogenic MEP
Conduction of these stimuli through the motor
pathways is monitored as peripheral nerve impulses,
electromyographic signals, or actual limb movements.
1996,lang et al- transient loss of amplitude (no neuro
deficit
Complete loss of tce-MEP)
More sensitive to anesthetic interface
74.
75. ELECTROMYOGRAPHY
Intraoperative EMG monitors motor cranial nerves,
spinal or peripheral nerves at risk by looking at either
the spontaneous or evoked CMAPs of the corresponding
effector muscles
normal - low frequency and amplitude
When the nerve is stretched or irritated, high-frequency
neurotonic discharges will be produced, which alerts the
surgical team of potential motor nerve damage
The absence of such discharges (i.e. a ‘‘negative
response’’) suggests either an intact nerve or total
denervation disrupting all nerve conduction.
76.
77.
78. Anaesthetic agents& EP
Opioid haveleast effecton SSEPs
Cortical SSEP is very sensitive to Potent inhalational agents ,
nitrous oxide.
Sub cortical SSEP is more resistant
MEPs is affected by
◦ nitrous+inhalational
◦ BZD, thiopentone
MR haveno effecton SSEPs or MEPs
79.
80. HYPOTHERMIA(lessthan36deg)
Long duration of surgery
Transfusion of blood &blood products
Hazards
◦ Impaired coagulationd/t Dec plateletfunction
◦ Wound infection(impairedimmune functanddec cutaneousbldflow)
◦ Delayed recovery(dec drug metabolism)
◦ Acid/base changes
◦ hypothermia reduces conduction velocity in peripheral
nerves and increases synaptic delay in awake and
anesthetized patients.
SSEP latency increases linearly with decreasing temperatures,
whereas the amplitude of the cortical SSEP is unchanged with
moderate hypothermia.
Prevention
◦ Monitoring ,warm fluids,warming blankets,warm irrigation solutions
84. Surgical factors Blood loss > 30 ml/kg
Surgical invasion to thoracic cavity
Surgical factors
◦ Blood loss > 30ml/kg
◦ Surgical invasion to thoracic cavity
85. Postoperative concerns
Paralysis
Pulmonary complications
(Pneumothorax/hydrothorax/atelectasis)
Pain management
Pulmonary function
Post op ventilation
Hyponatraemia
Bleeding & coagulation abnormalities
86. PAINMANAGEMENT(multimodal analgesia)
For frequent physiotherapy and early mobilization and thus reduce
post op resp complications.
Parental opioid (48 hours)
◦ continuous infusion/iv PCA
NSAIDs
◦ Opioid sparing effect
◦ Reports that ketorolac inhibits spinal fusion
Epidural infusion(paravertebral catheter)- anterior correction
◦ Local anaesthetic + opioid infusion
Intrathecal opioid
◦ Morphine 5 – 10µg/kg
87. OPTIMISATION OFPULMONARY
STATUS
Incentive spirometry
-Coughing and deep breathing should be
encouraged
-Bronchodilators therapy ifreactive airway disease also present
-Adequate analgesia
Others-
Maintain urineoutput >0.5ml/kg/hr
Compression stockings/ pneumatic legpumpsforDVTprophylaxis
88. summary
• In Kyphoscoliosis there is involvement of various
organ systems.
• Anaesthesia is often needed for corrective
orthopaedic surgery.
• A detailed preanaesthetic assessment and optimization
of the respiratory and cardiovascular systems is
important.
• Intraoperative considerations are monitoring,
temperature and fluid balance maintenance, positioning,
spinal cord integrity monitoring and blood conservation.
• Post operative concerns- intensive care, respiratory
care and pain therapy