This document provides information about conducting an eye exam, including:
1) Taking a case history to understand a patient's vision needs, eye health history, and general health conditions.
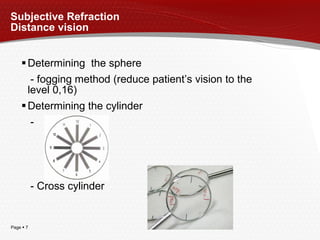
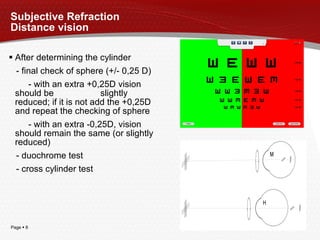
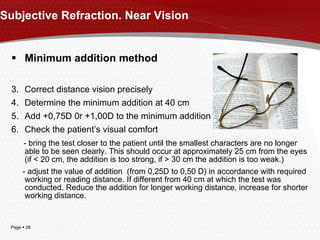
2) Performing objective and subjective refraction tests to determine a patient's prescription for distance and near vision.
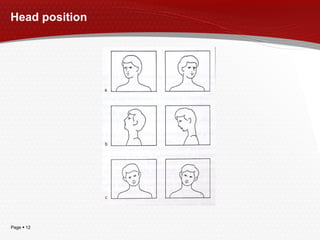
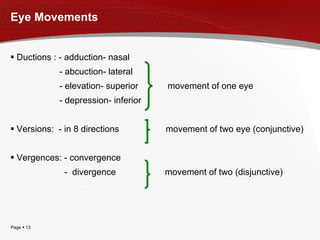
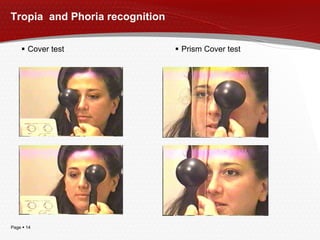
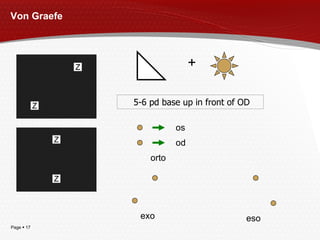
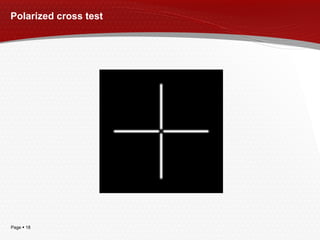
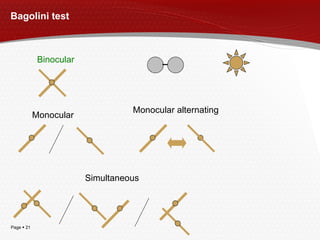
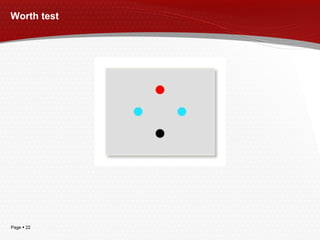
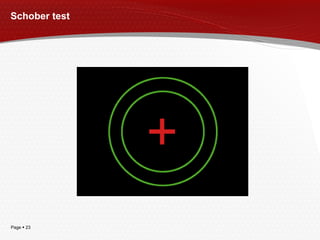
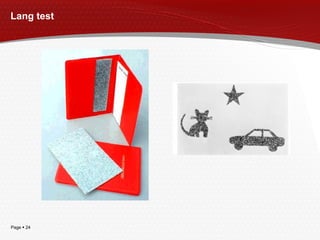
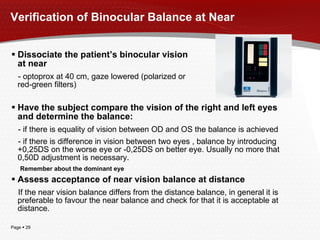
3) Evaluating binocular vision by testing motor and sensory functions like eye movements, stereopsis, and fusional reserves.
4) Prescribing corrective lenses or prisms as needed based on the refraction and binocular vision results.
![Refraction Author: Irina Jagiloviča e-mail: [email_address] www: www.optometristiem.lv](https://image.slidesharecdn.com/refraction-090626140442-phpapp01/85/Refraction-1-320.jpg)
![Refraction Author: Irina Jagiloviča e-mail: [email_address] www: www.optometristiem.lv](https://image.slidesharecdn.com/refraction-090626140442-phpapp01/75/Refraction-1-2048.jpg)