Downloaded 411 times


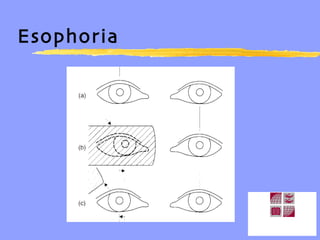

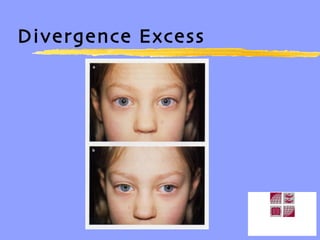







Ocular deviations can be classified as heterophorias or heterotropias. Heterophorias are latent deviations that are suppressed by fusion, while heterotropias are manifest deviations. Specific types of heterophorias include esophoria, exophoria, hyperphoria, and hypophoria. It is important to record the size of any deviation in prism diopters and the distance at which the test was performed. Heterotropias can be incomitant, meaning the deviation varies with gaze direction, or concomitant, where the deviation remains constant. Incomitant strabismus is often paralytic in origin while concomitant may have an accommodative element.













































































