




![Inserting an NG tubeMark this distance on the tubing with tape, or note the marking already on the tube. (Average measurements for an adult range from 22” to 26” [56 to 66 cm].) It may be necessary to add 2” (5.1 cm) to this measurement in tall individuals to ensure entry into the stomach.To determine which nostril will allow easier access, use a penlight and inspect for a deviated septum or other abnormalities. Ask the patient if she ever had nasal surgery or a nasal injury.24](https://image.slidesharecdn.com/nasogastrictubeinsertion-100622130125-phpapp01/85/Nasogastric-Tube-Insertion-48-320.jpg)


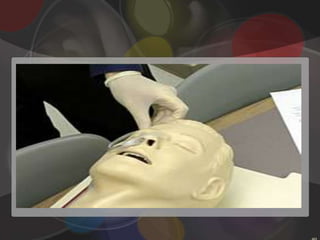
This document discusses the procedure for nasogastric tube insertion and removal. It describes the types of NG tubes used, the equipment needed, and steps to take to ensure proper placement. Key steps include lubricating the tube, having the patient swallow as it's advanced, checking placement by aspirating stomach contents and using a pH test strip, and securing the tube to the nose with tape. For removal, the tube is flushed, untaped, and gently withdrawn while having the patient hold their breath.





















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















