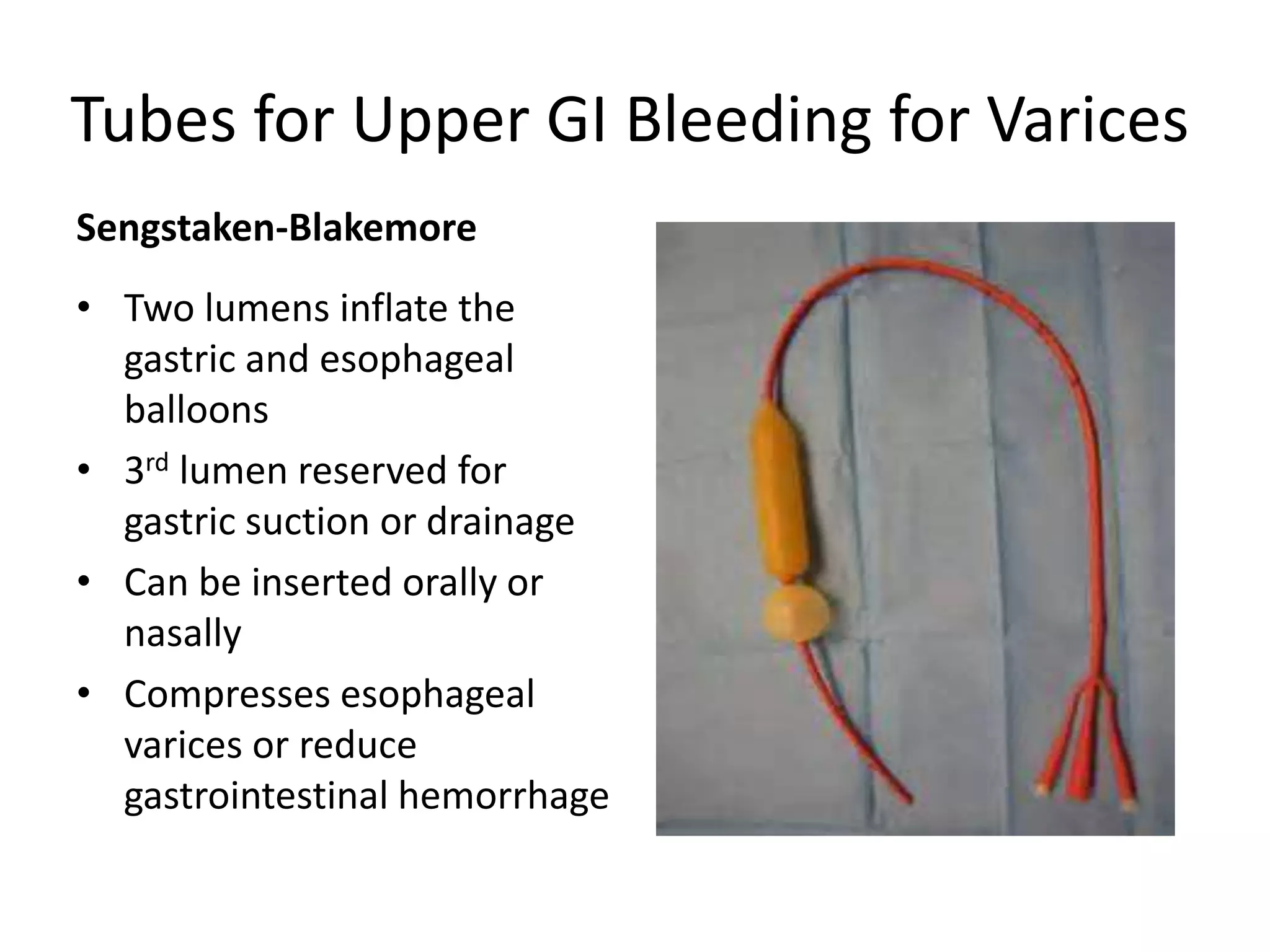
This document discusses various types of gastric tubes including Salem sump tubes, Levin tubes, Moss Mark IV tubes, Miller-Abbott tubes, Sengstaken-Blakemore tubes, PEG tubes, and J-tubes. It provides details on their uses, placement, care, and contraindications. Guidelines are provided for enteral feeding administration and maintenance as well as parenteral nutrition indications and considerations.