Downloaded 255 times

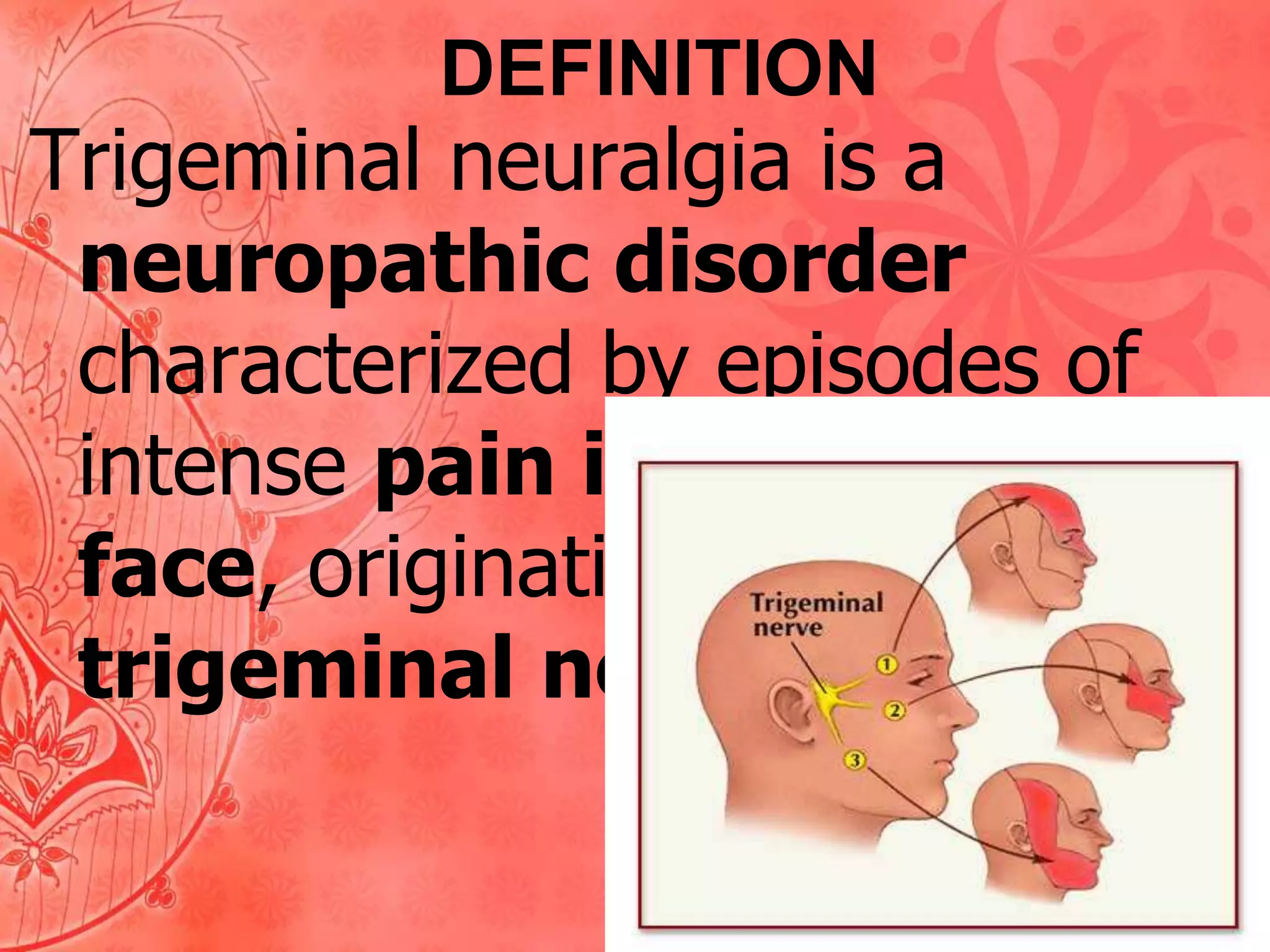
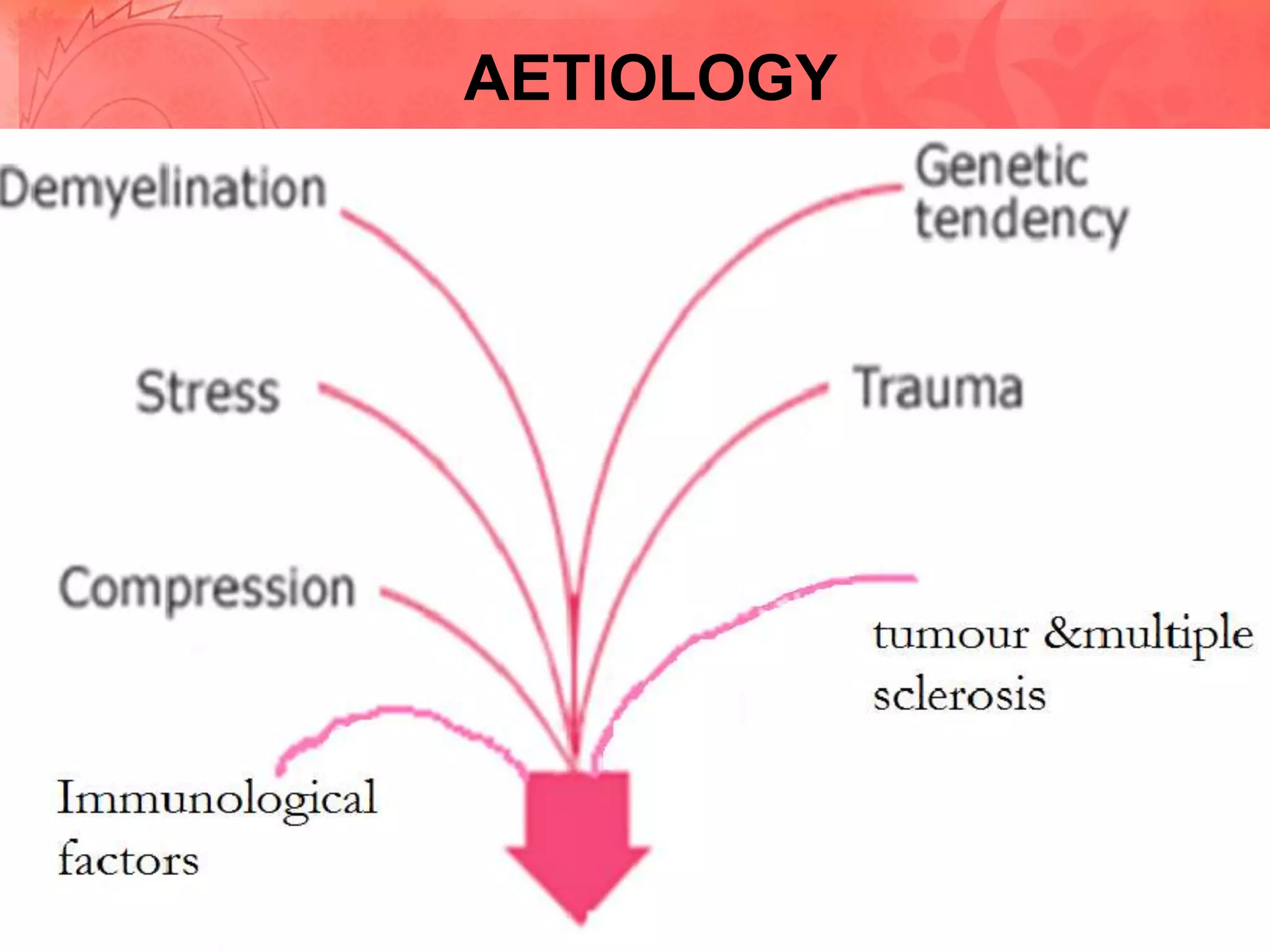
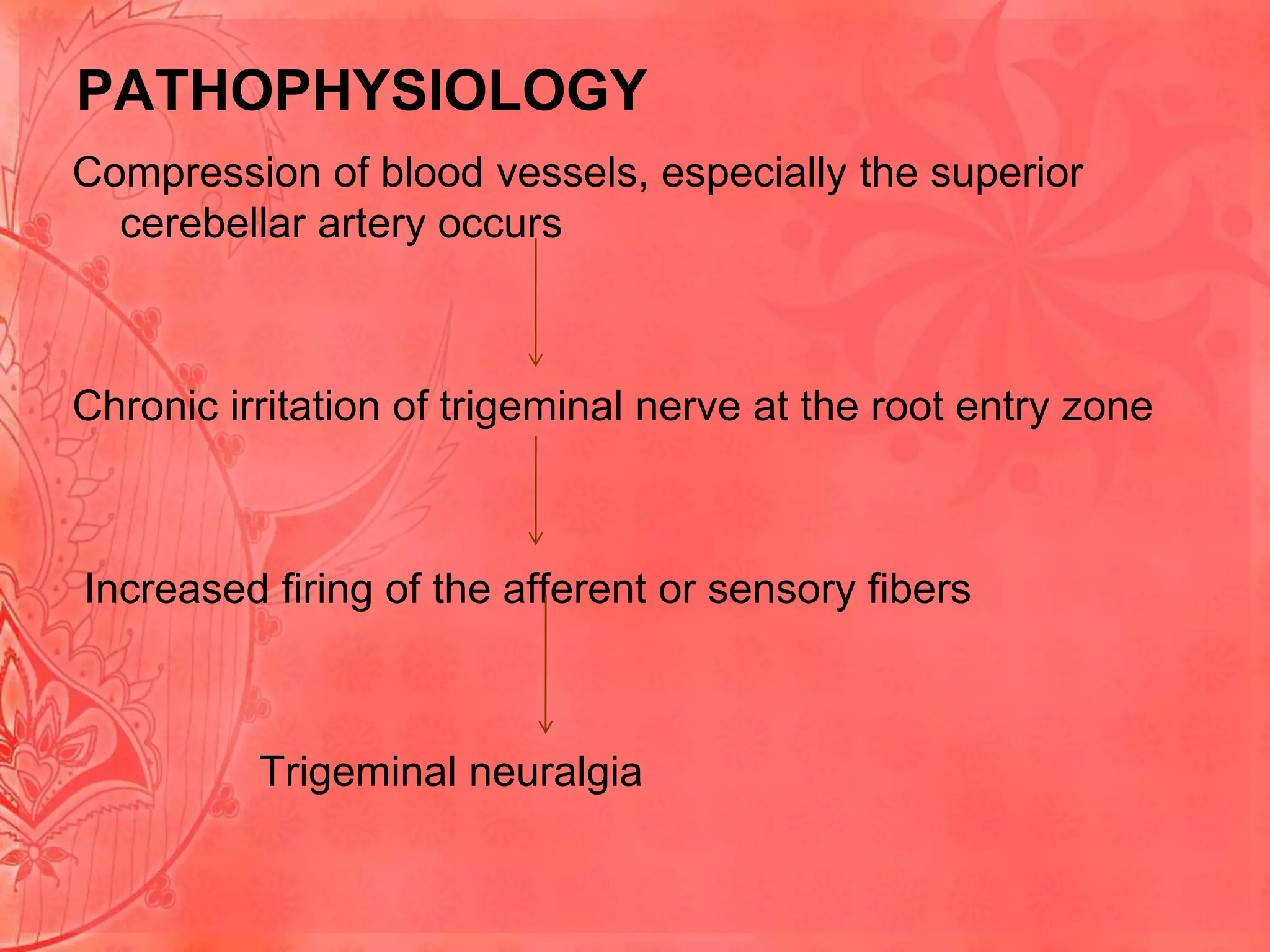




Trigeminal neuralgia is a neuropathic disorder characterized by episodes of intense facial pain originating from the trigeminal nerve. Common causes include compression of blood vessels like the superior cerebellar artery which can irritate the trigeminal nerve root. Symptoms include excruciating burning or shock-like pain in areas supplied by the trigeminal nerve. Diagnosis involves examinations, imaging tests and ruling out other conditions. Treatment options include medications like carbamazepine or surgical procedures like microvascular decompression to relieve pressure on the nerve. Recurrence of trigeminal neuralgia is common if initially caused by veins, with regrowth of veins being a primary reason for returned symptoms within one year. Further microvascular decompression


























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






