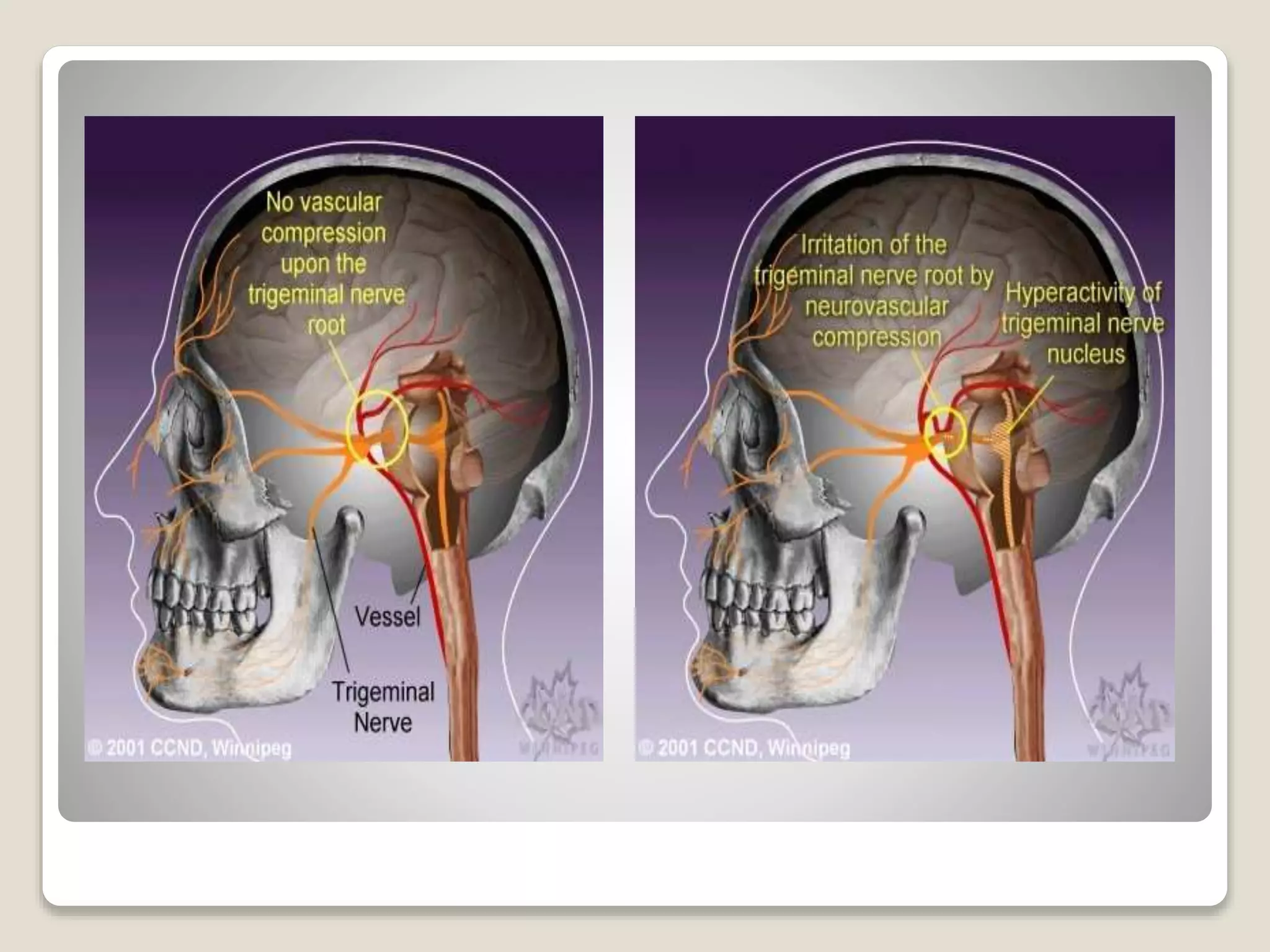
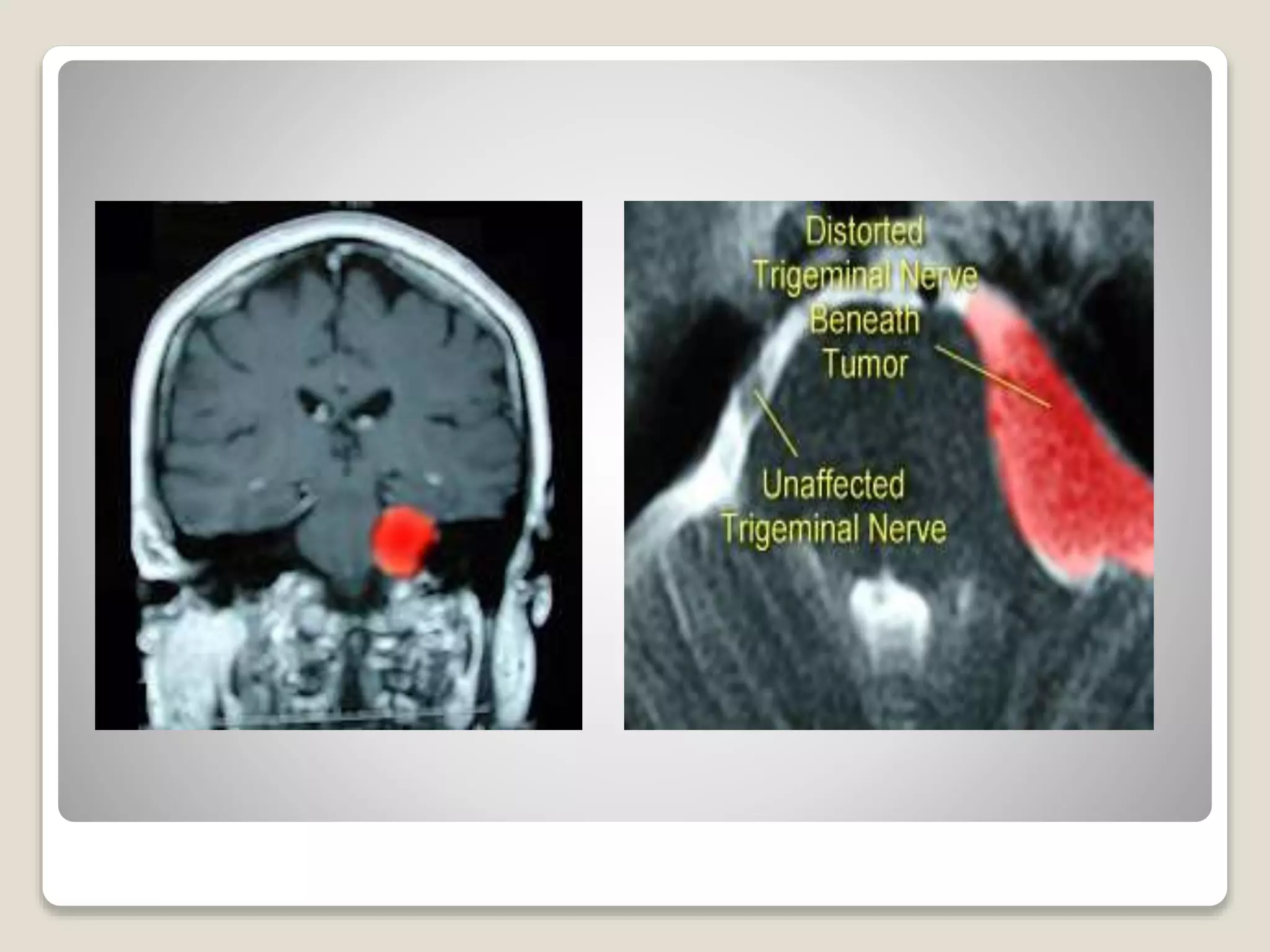
Trigeminal neuralgia is a neuropathic disorder causing episodes of intense pain in the face. It is characterized by brief, severe electric shock-like pains triggered by mundane stimuli like washing or talking. It is caused by a blood vessel compressing the trigeminal nerve root. Treatments include carbamazepine and other anticonvulsants as first-line medical options or microvascular decompression surgery to relieve nerve compression.




























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)






