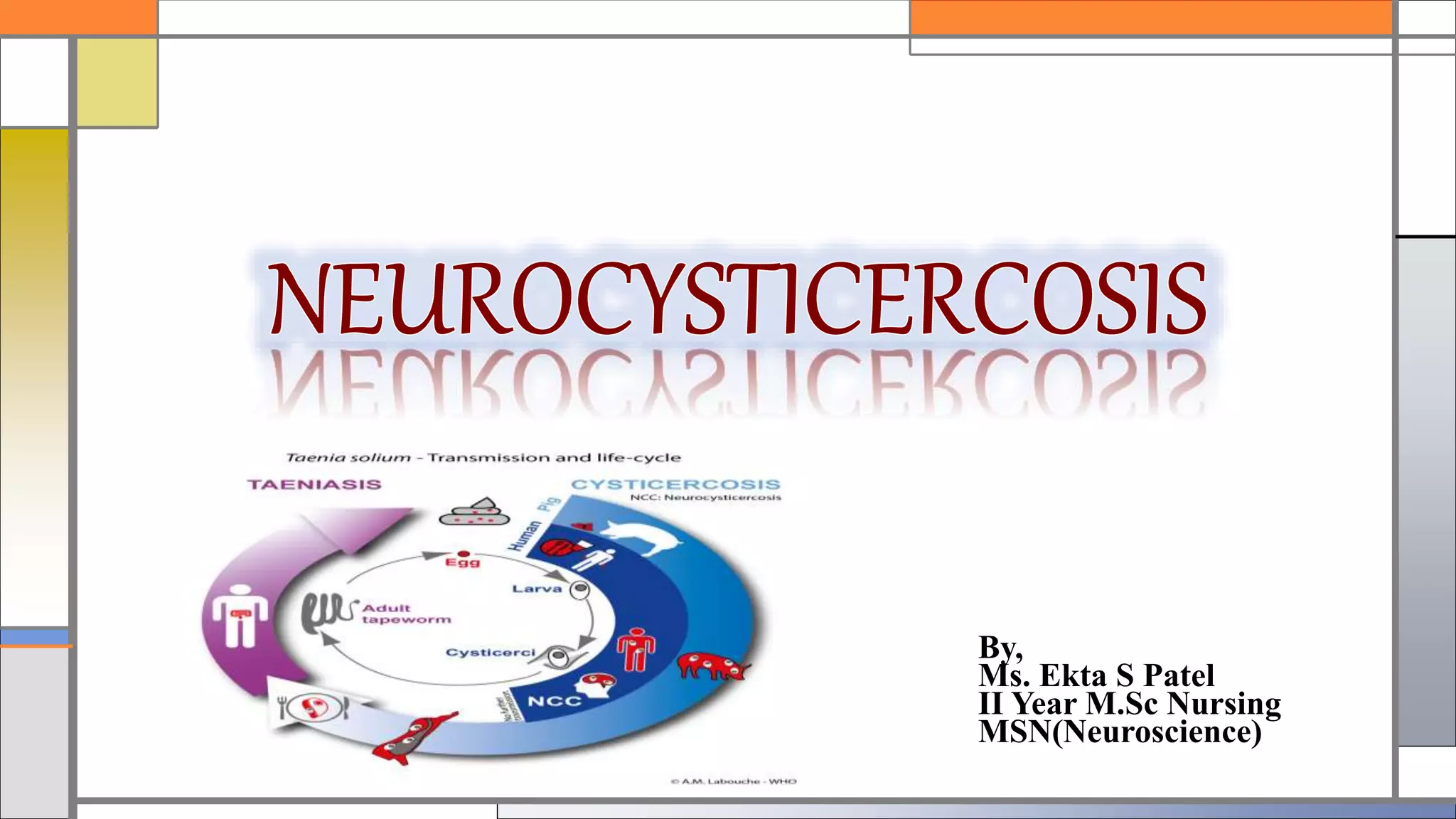
Neurocysticercosis is a condition caused by the larva of the pork tapeworm (Taenia solium) becoming encysted in human brain tissue. It is most common in developing countries where sanitation is poor and pigs have access to human feces. Common symptoms include seizures, focal neurological deficits, increased intracranial pressure, and hydrocephalus. Diagnosis involves history, physical exam, CT/MRI imaging, and stool studies. Treatment consists of antiparasitic medications like praziquantel or albendazole as well as surgery for complications like hydrocephalus. Nursing care focuses on monitoring for increased intracranial pressure and seizures while providing patient education.

























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


