Downloaded 1,547 times
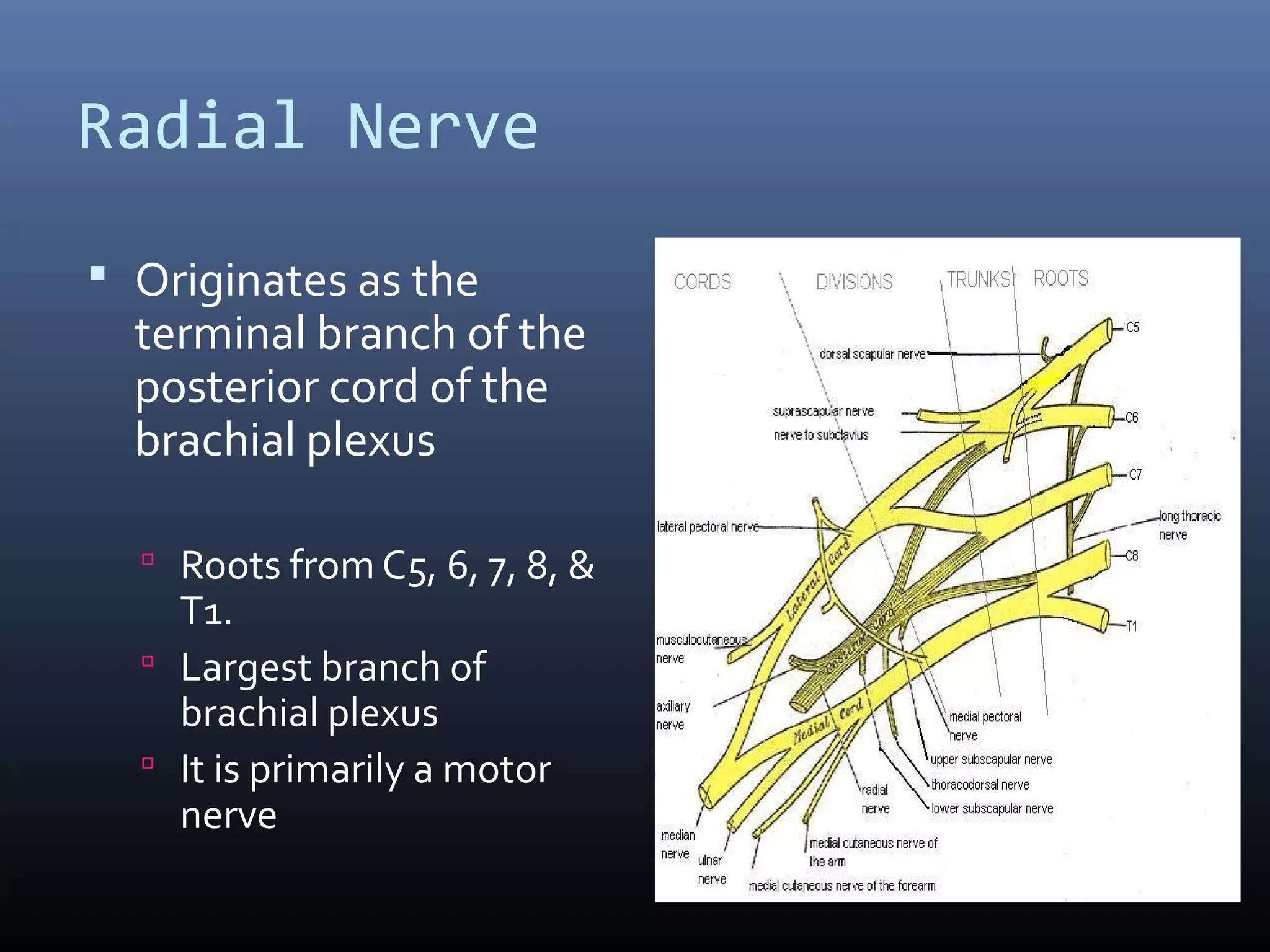
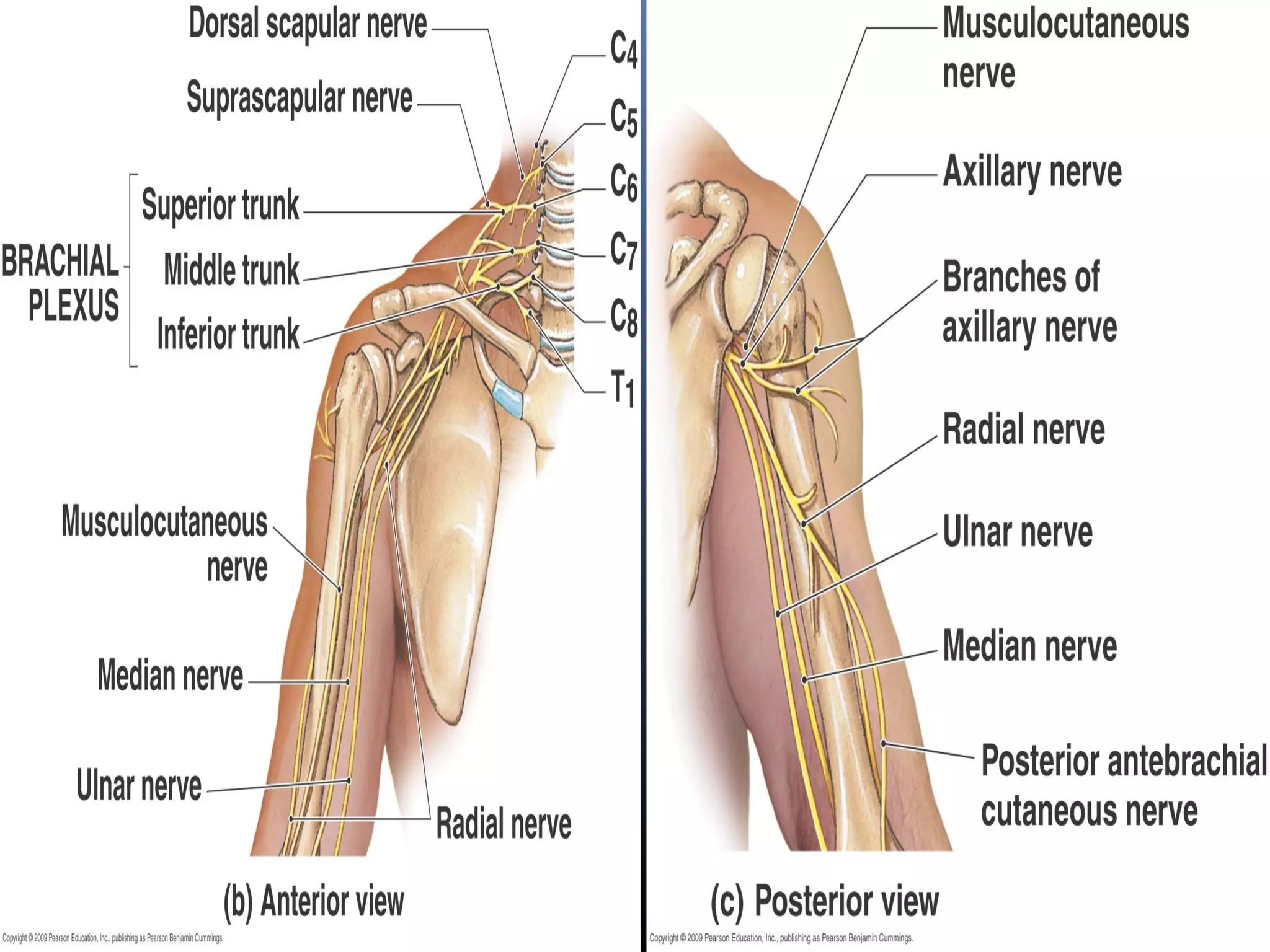
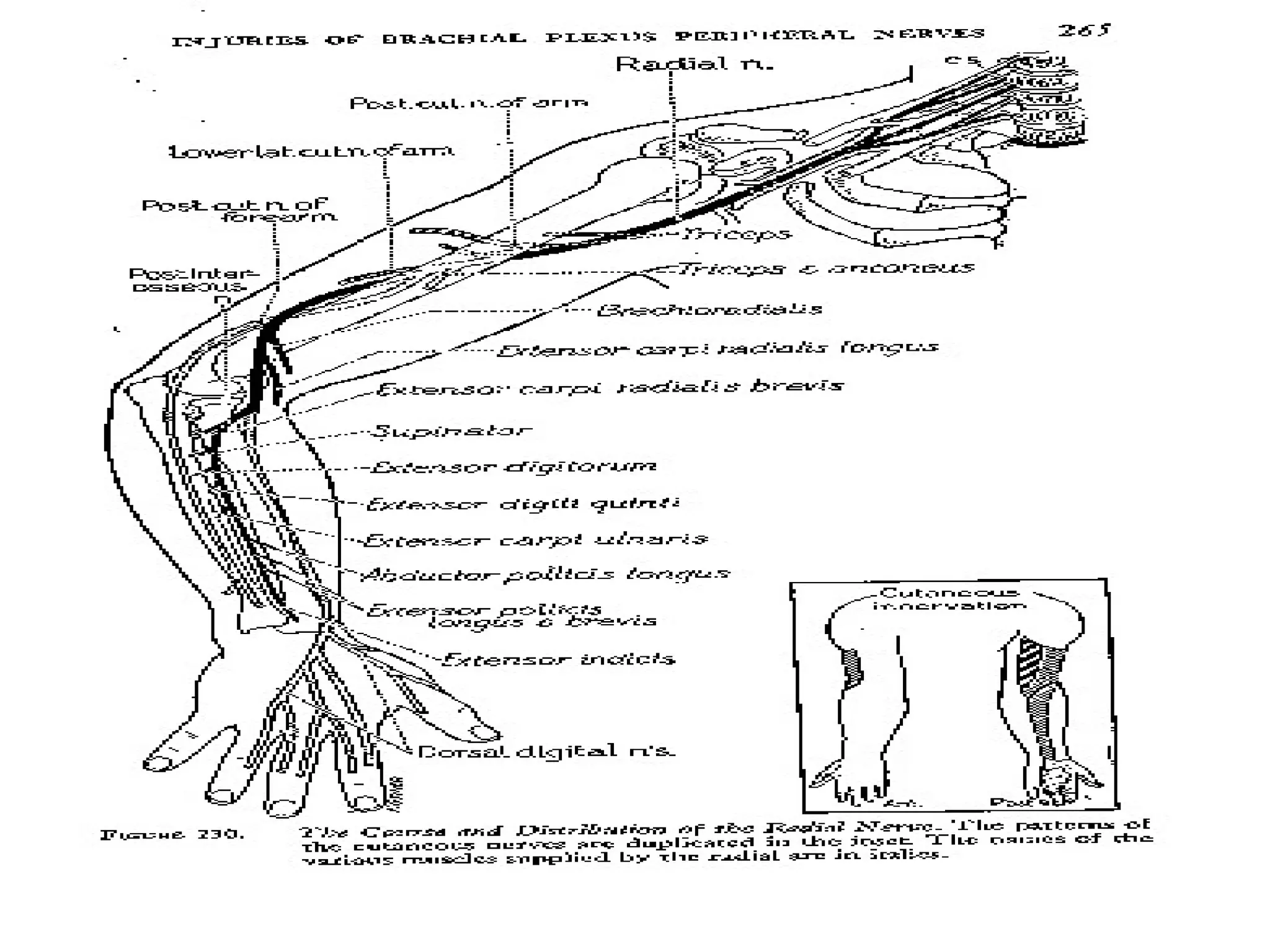
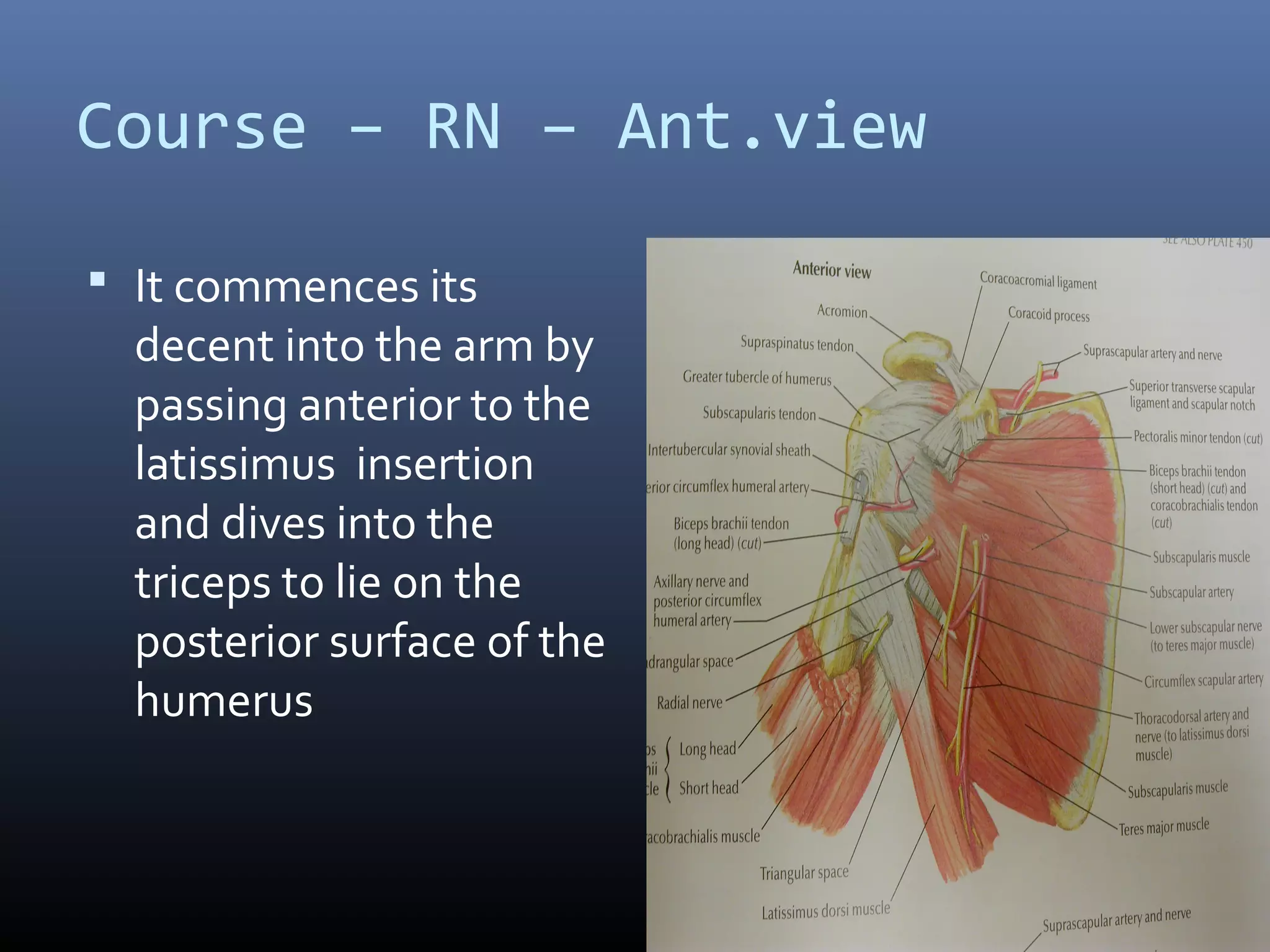
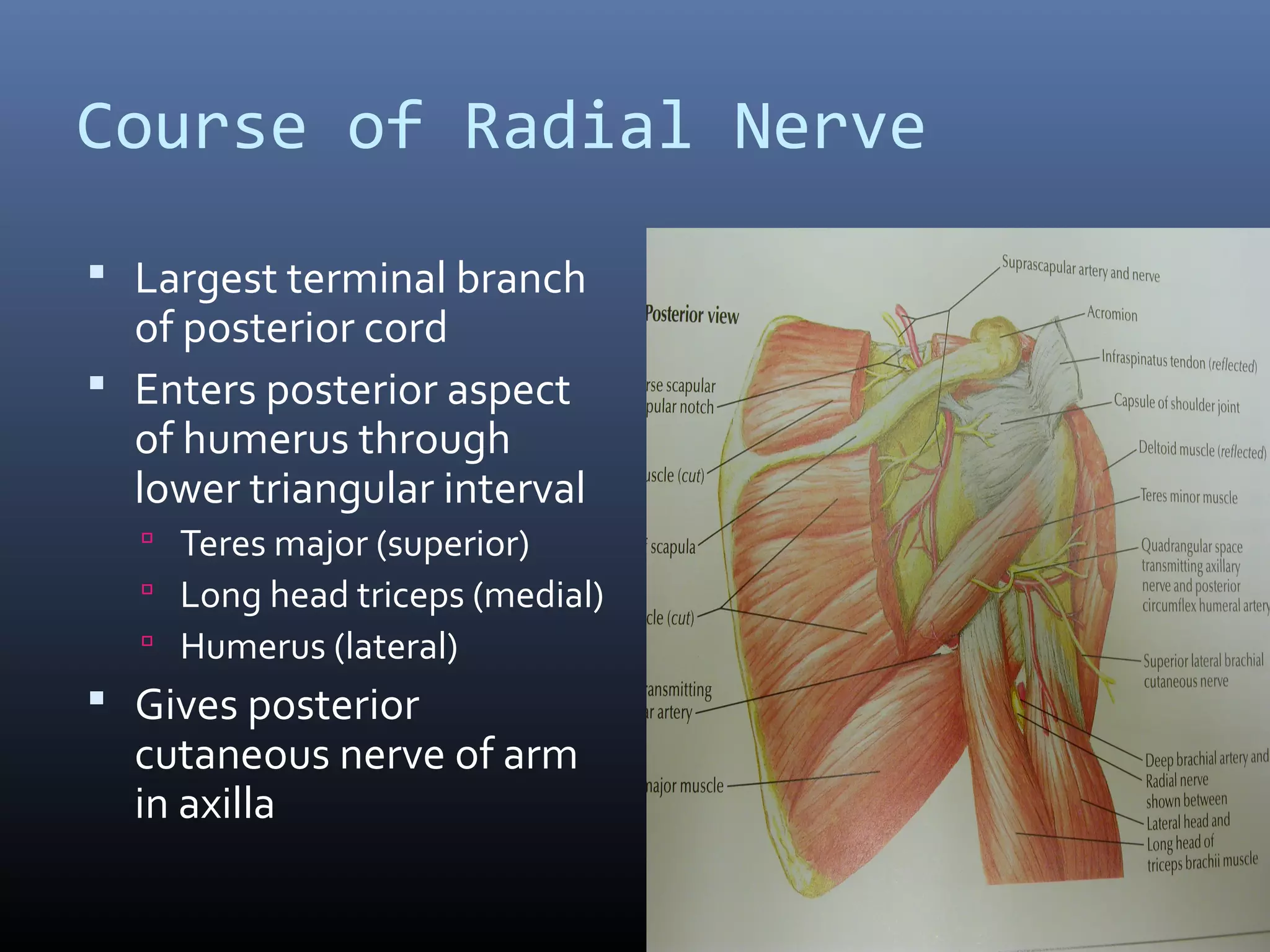
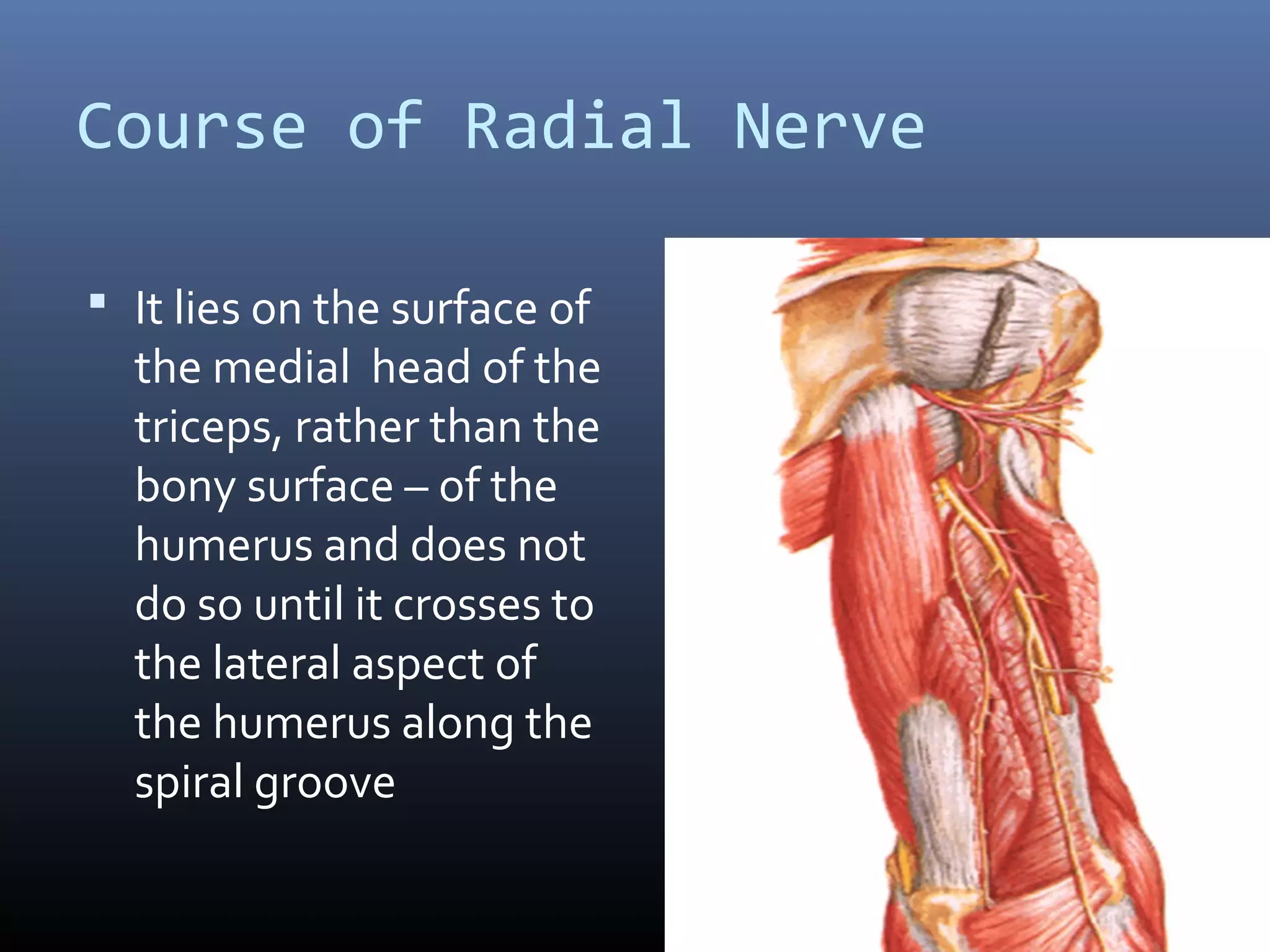

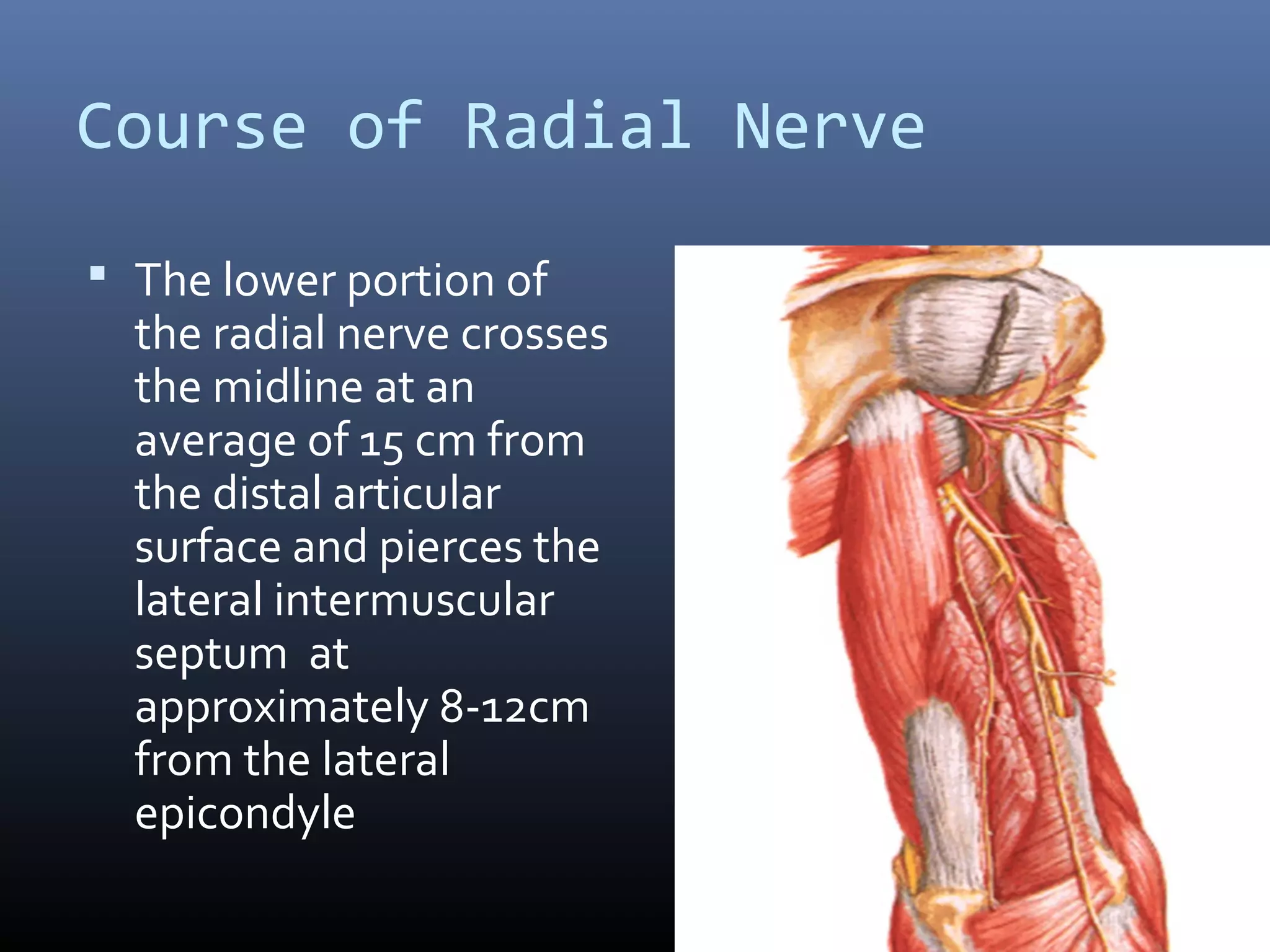
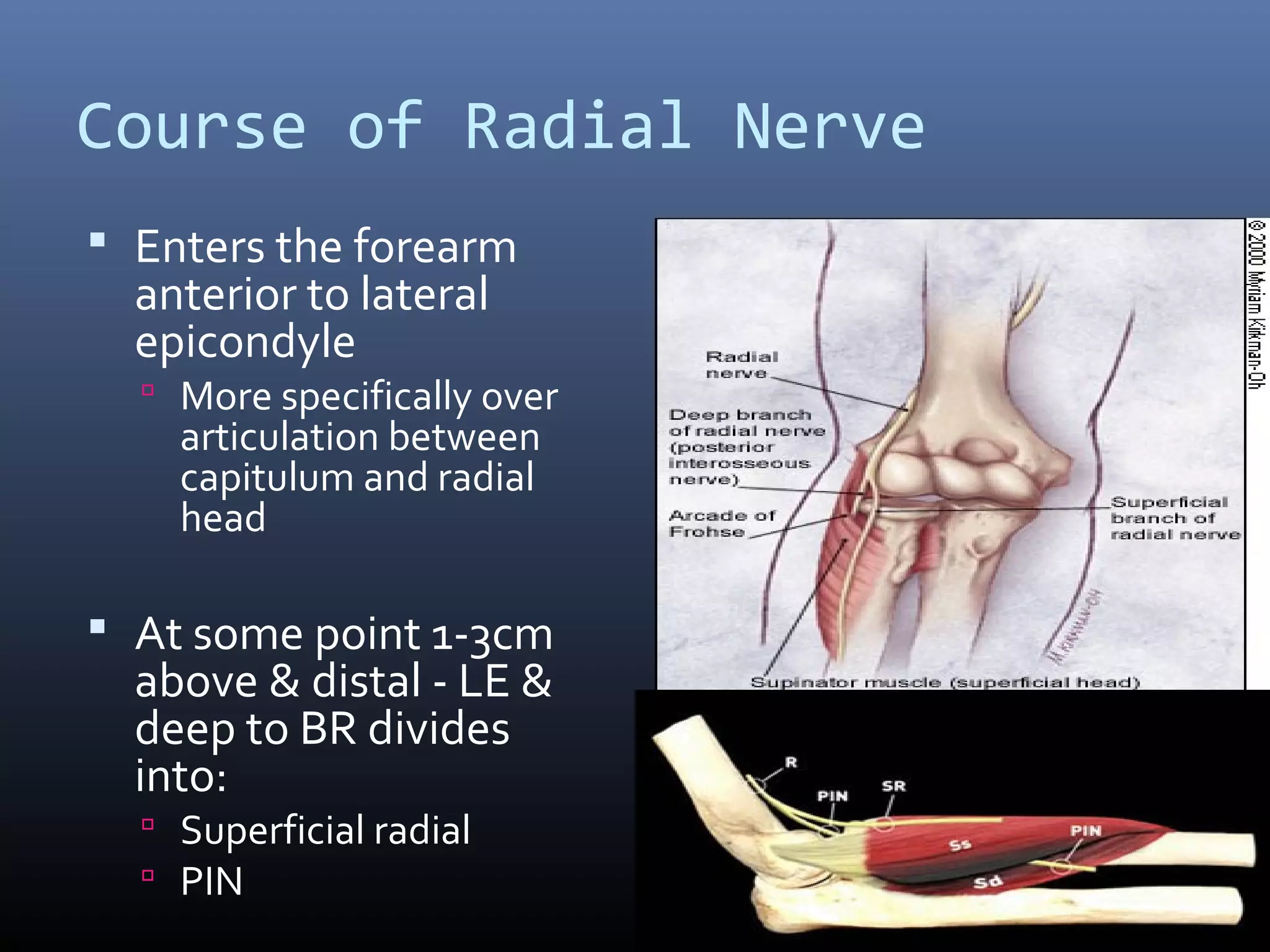
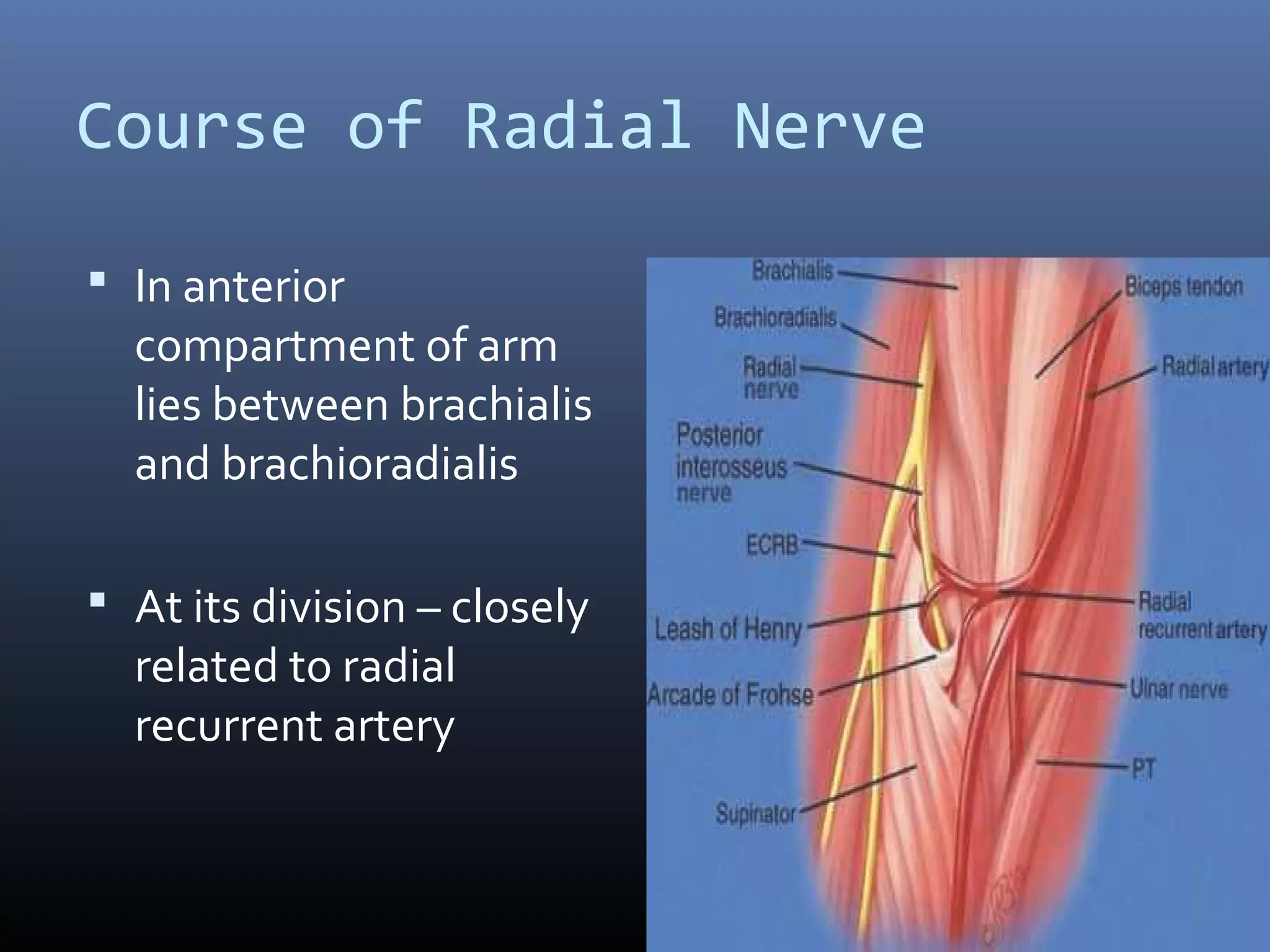
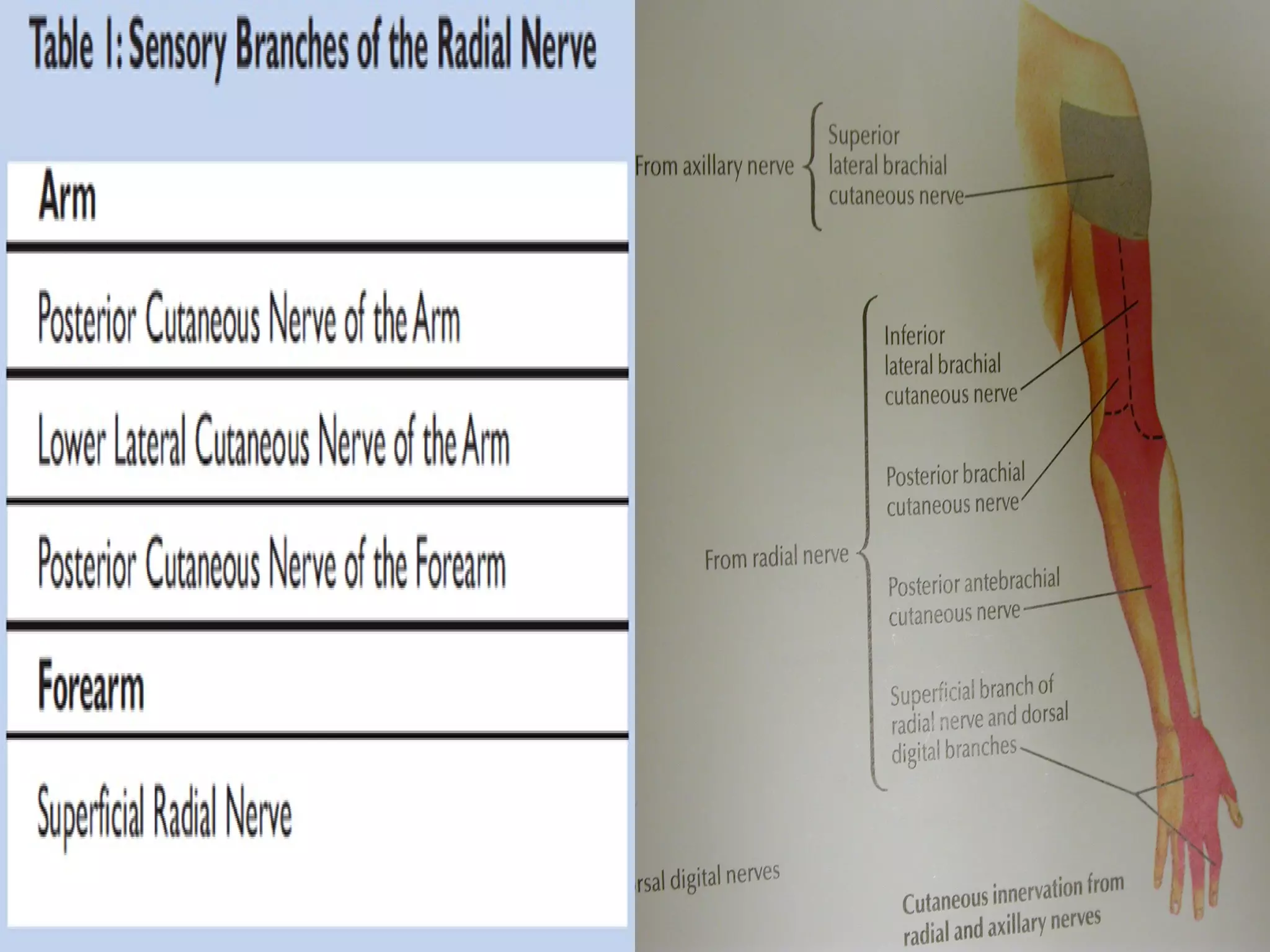
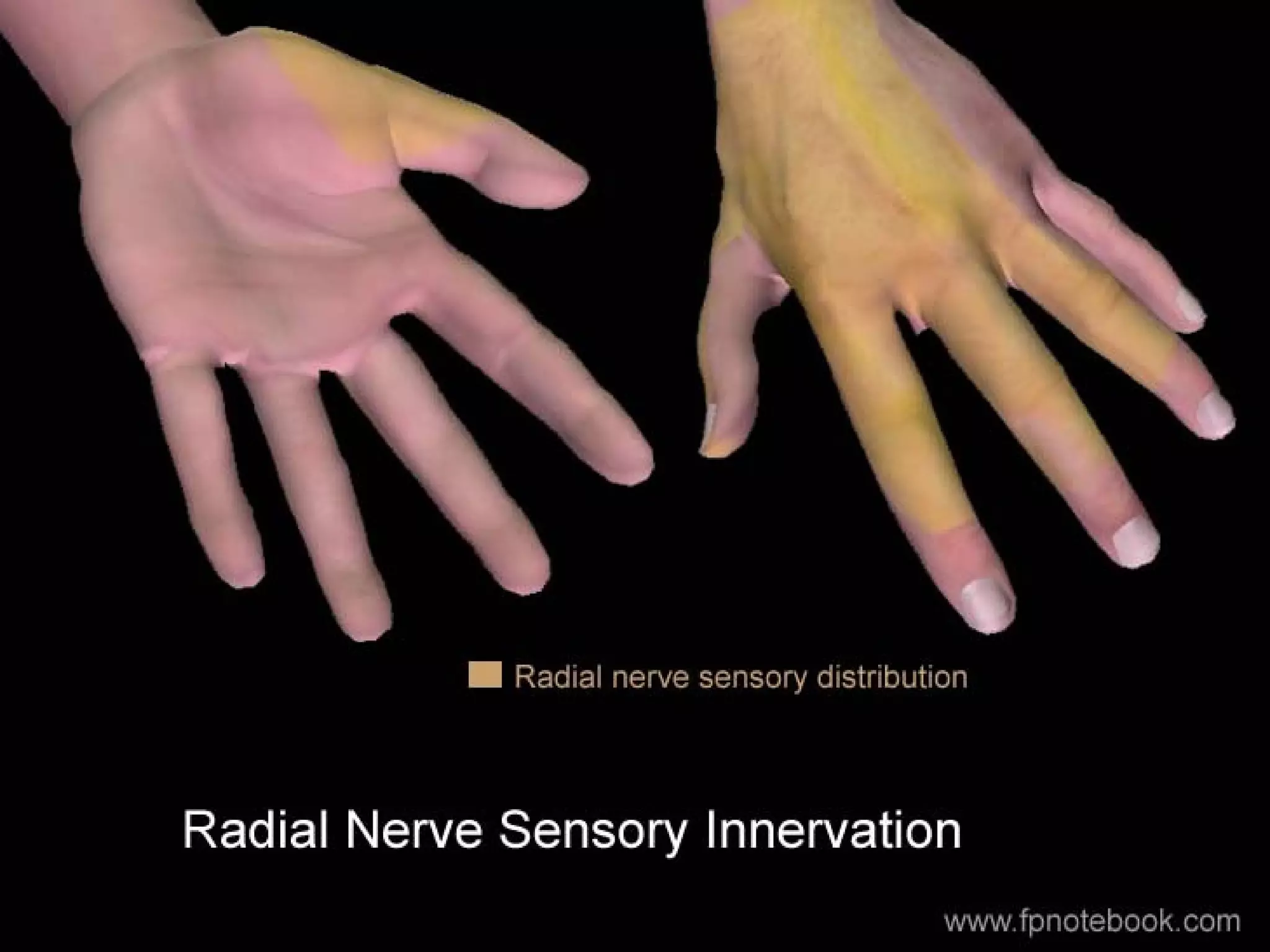
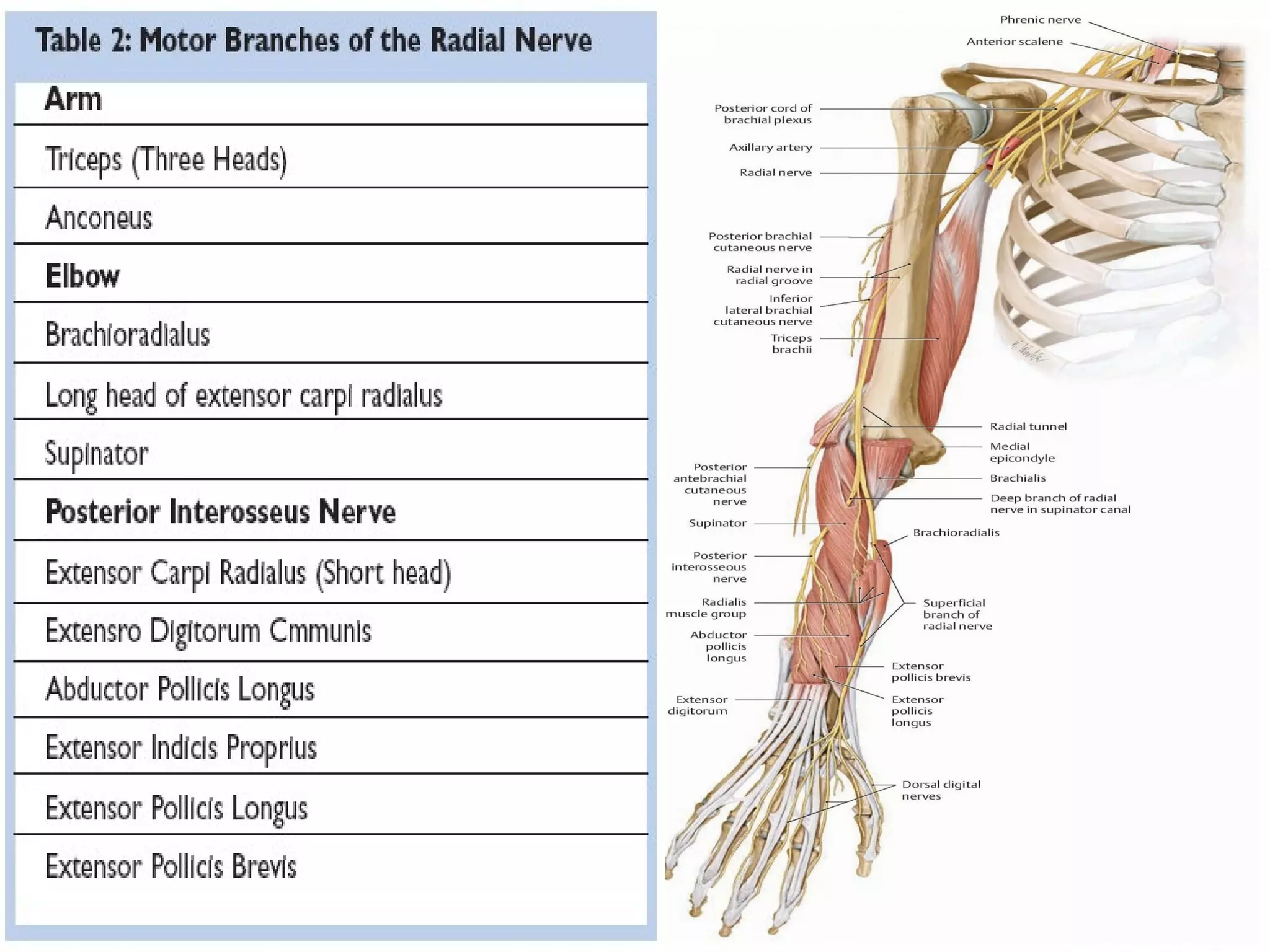
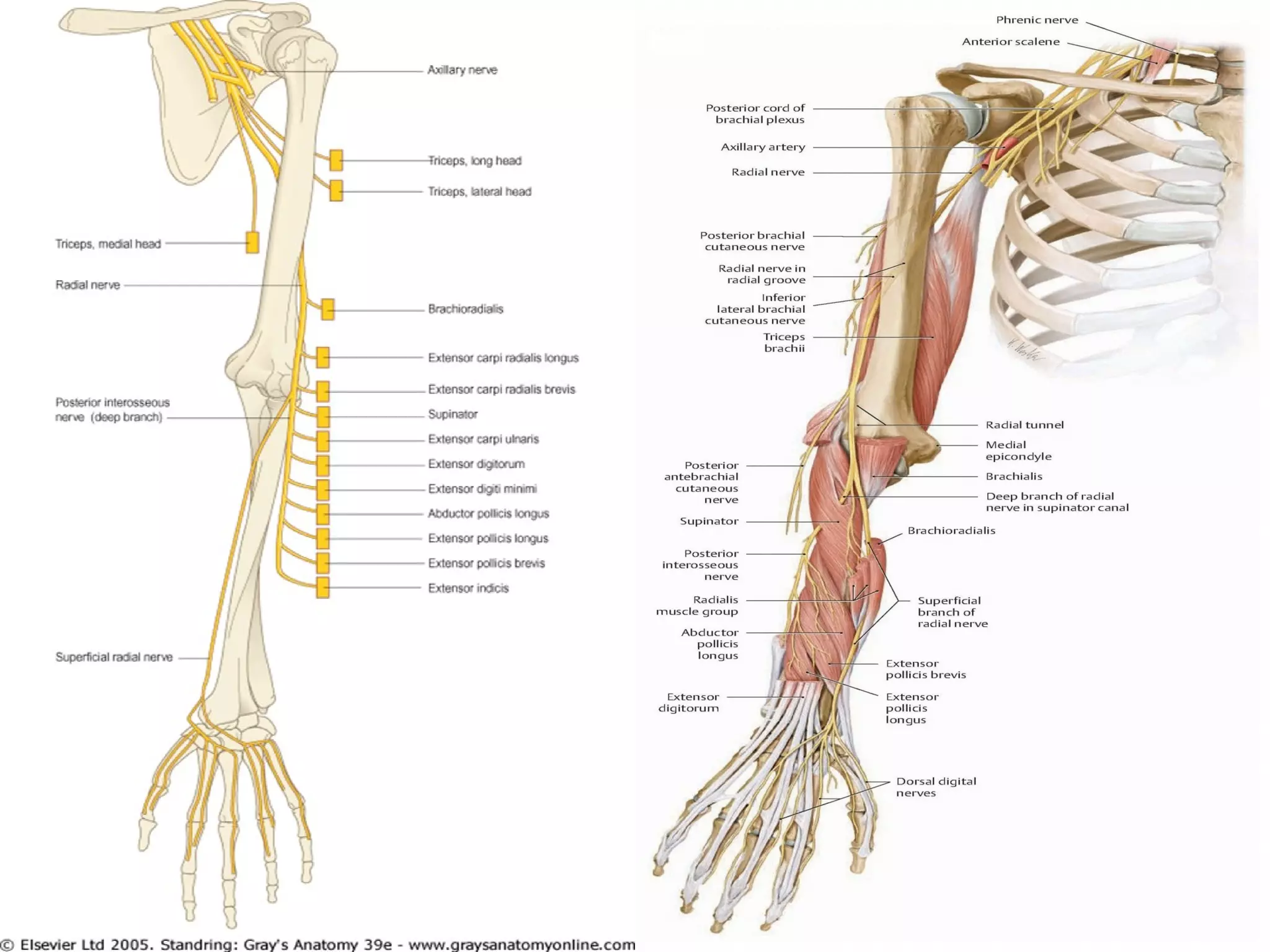
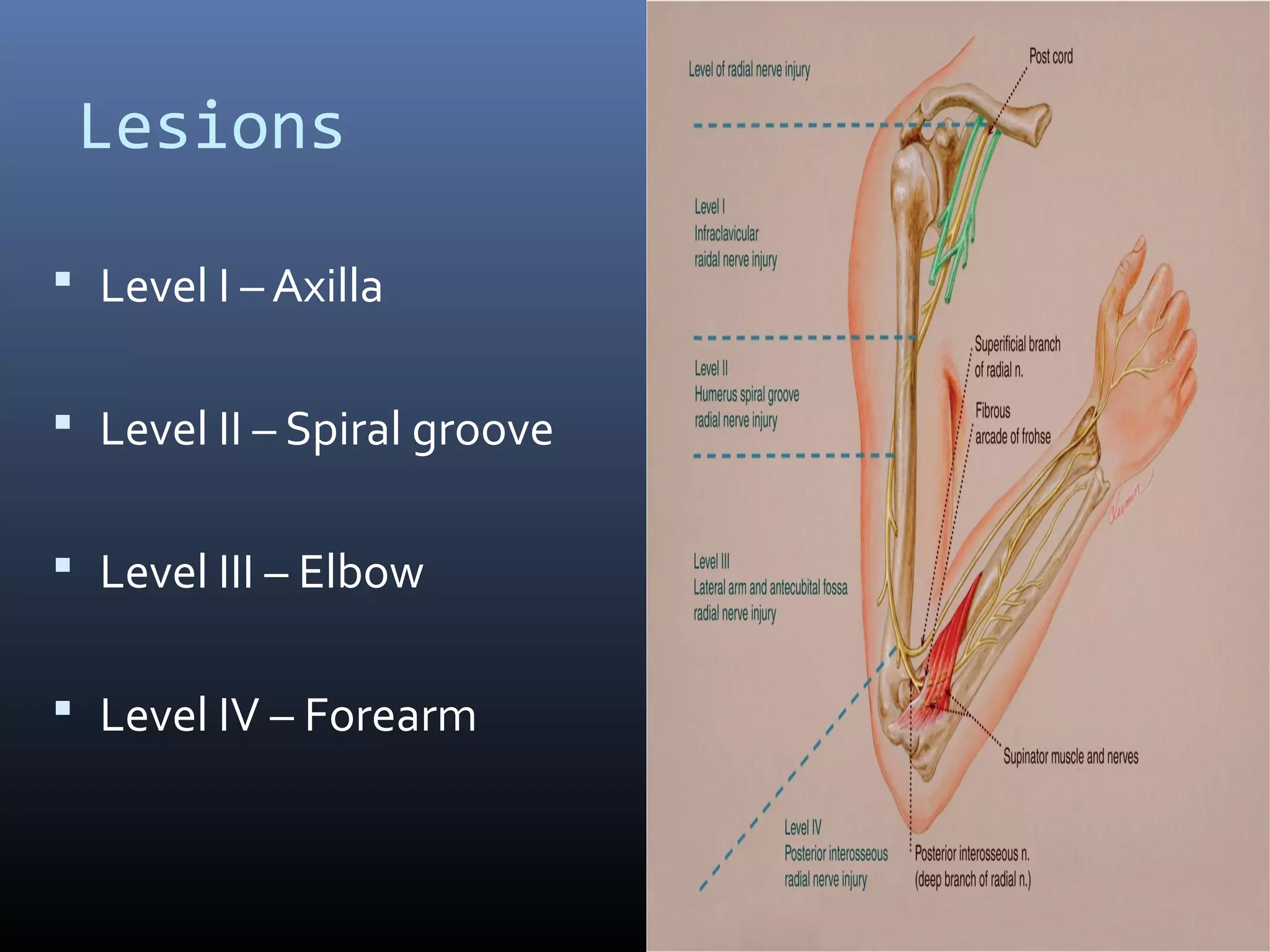
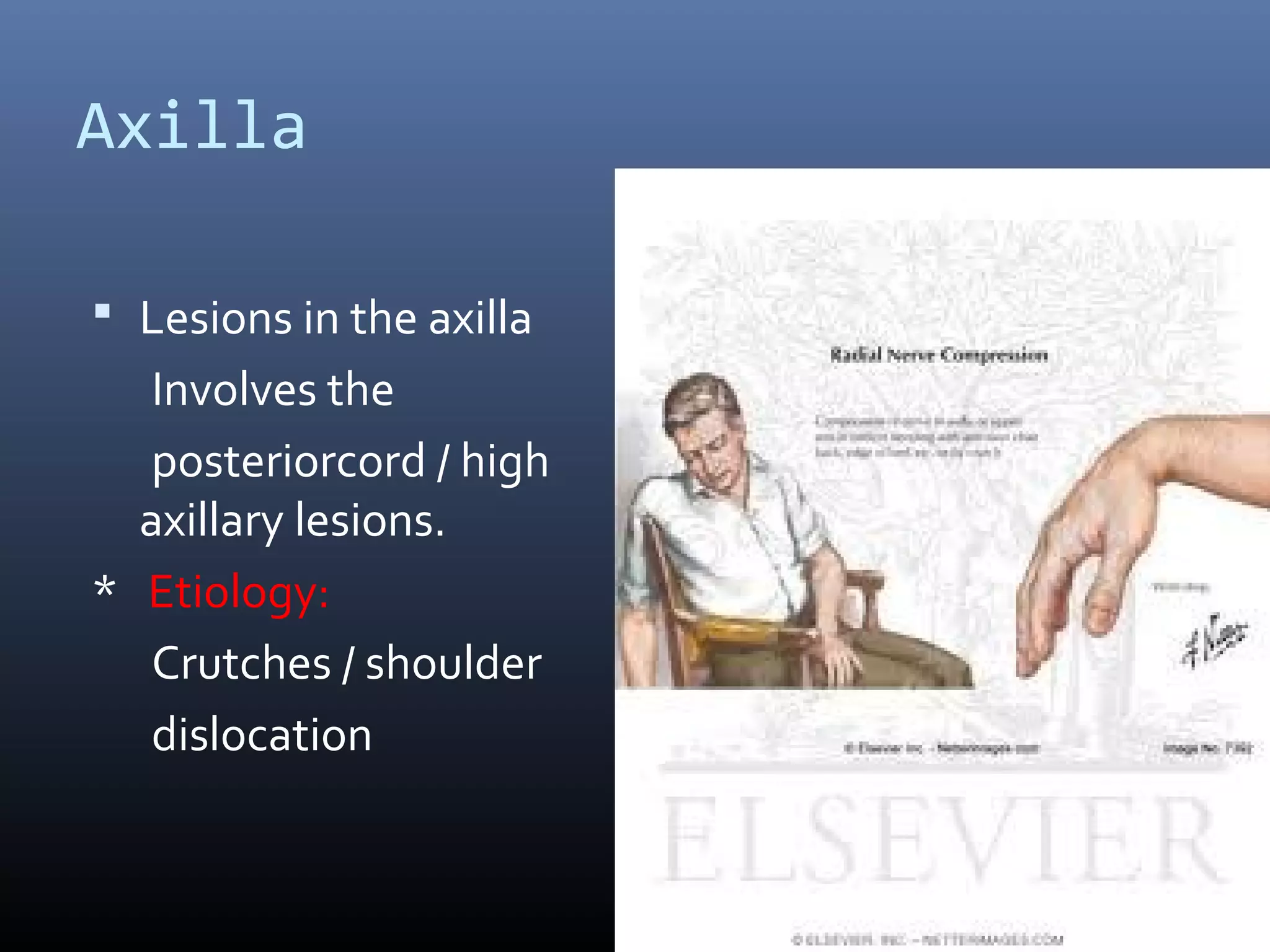
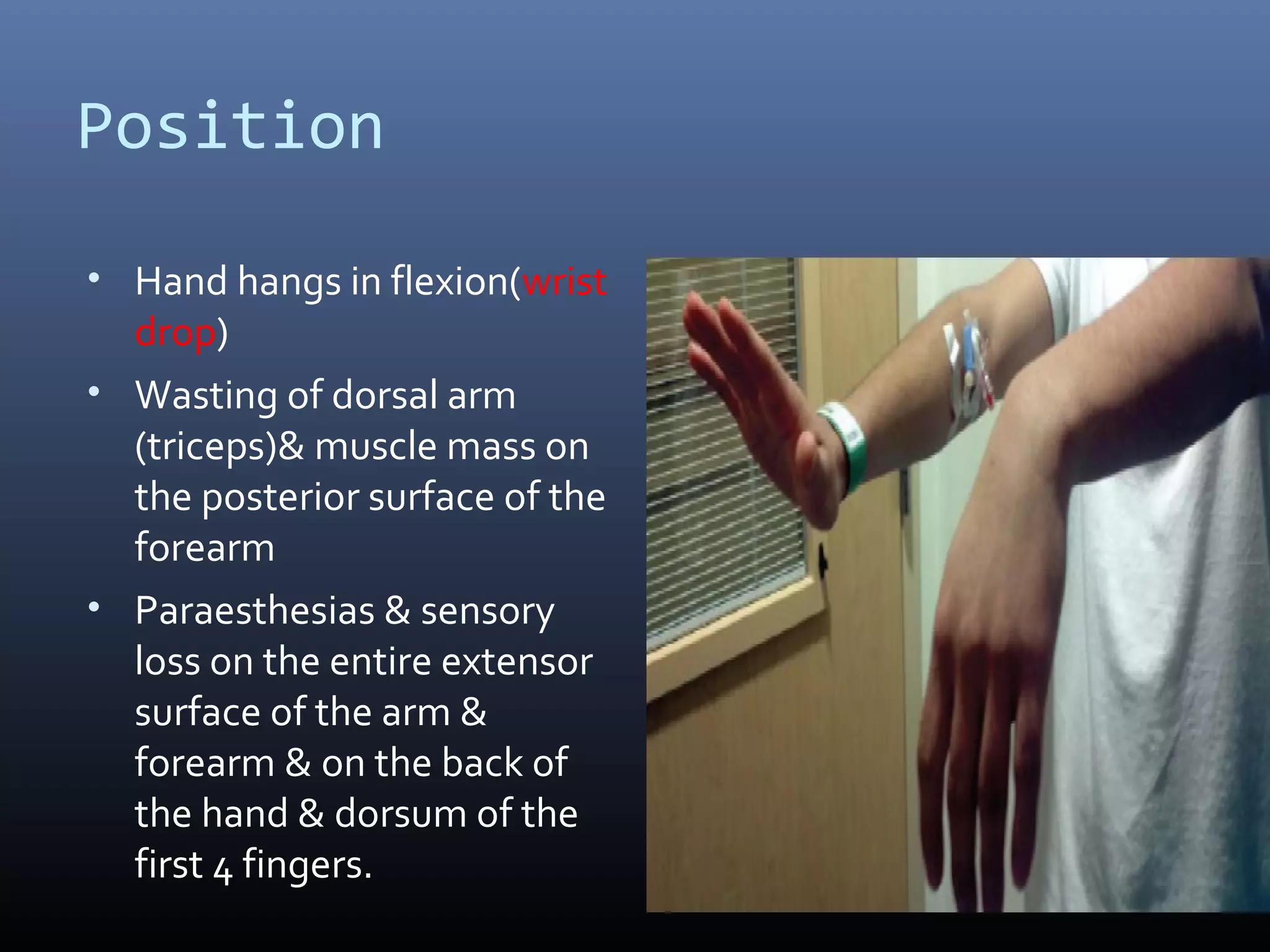

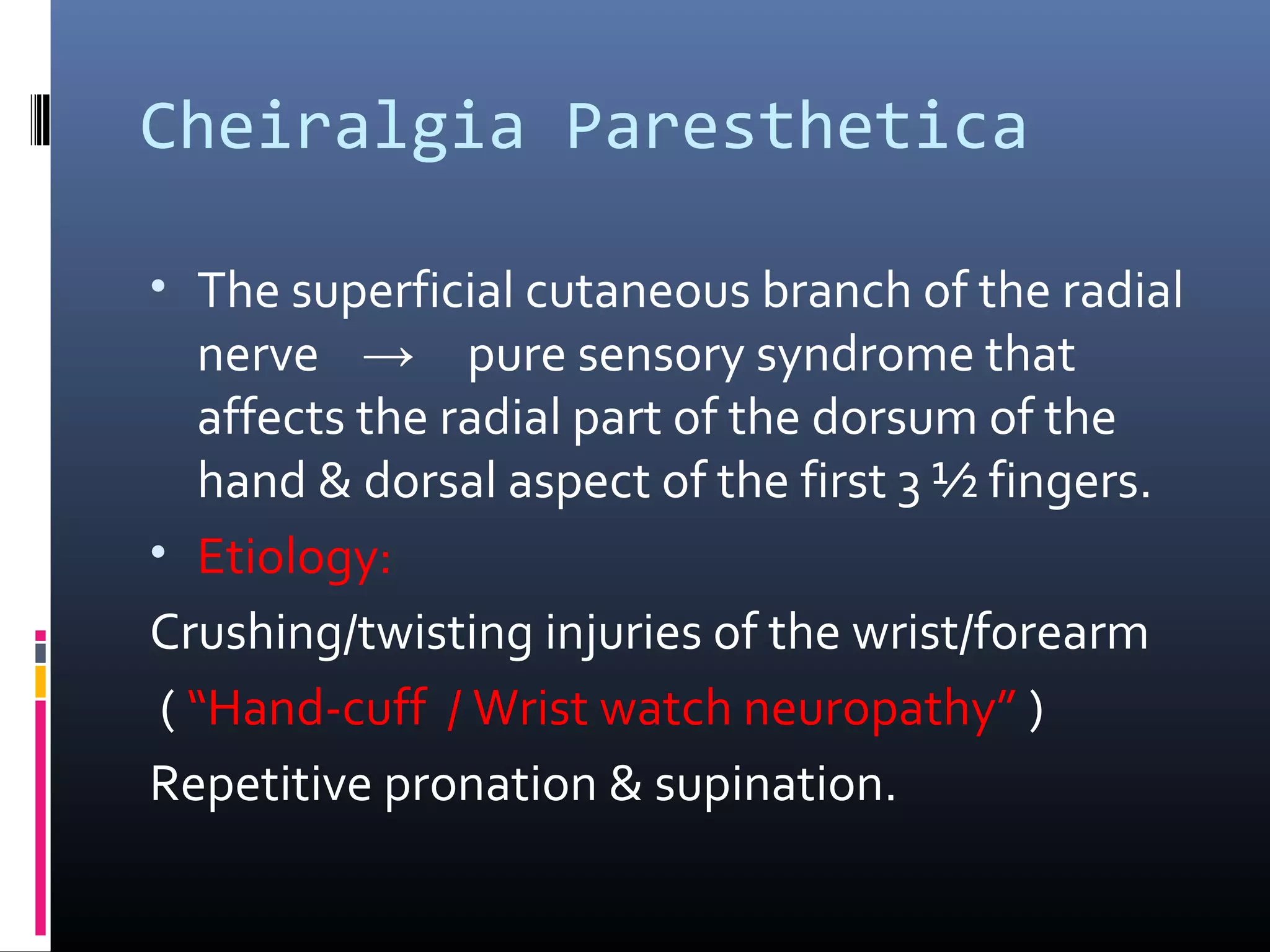



The radial nerve is the largest branch of the brachial plexus, originating from the posterior cord and providing motor function to the forearm and arm's extensor muscles. Its course includes passing behind the axillary artery and lying in the spiral groove of the humerus, where it becomes vulnerable to injury, resulting in conditions like wrist drop if damaged. Additionally, injuries at different levels, such as the axilla or spiral groove, yield distinct clinical manifestations, affecting elbow extension and sensory functions.






















































![RADIAL NERVE PALSY[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/radialnervepalsy1-220928130238-5944f60b-thumbnail.jpg?width=640&height=640&fit=bounds)






![Advanced Trauma Life Support [ATLS] and Triage](https://cdn.slidesharecdn.com/ss_thumbnails/atlstriage-251212075759-fbe88f4f-thumbnail.jpg?width=640&height=640&fit=bounds)






































