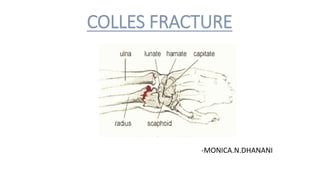
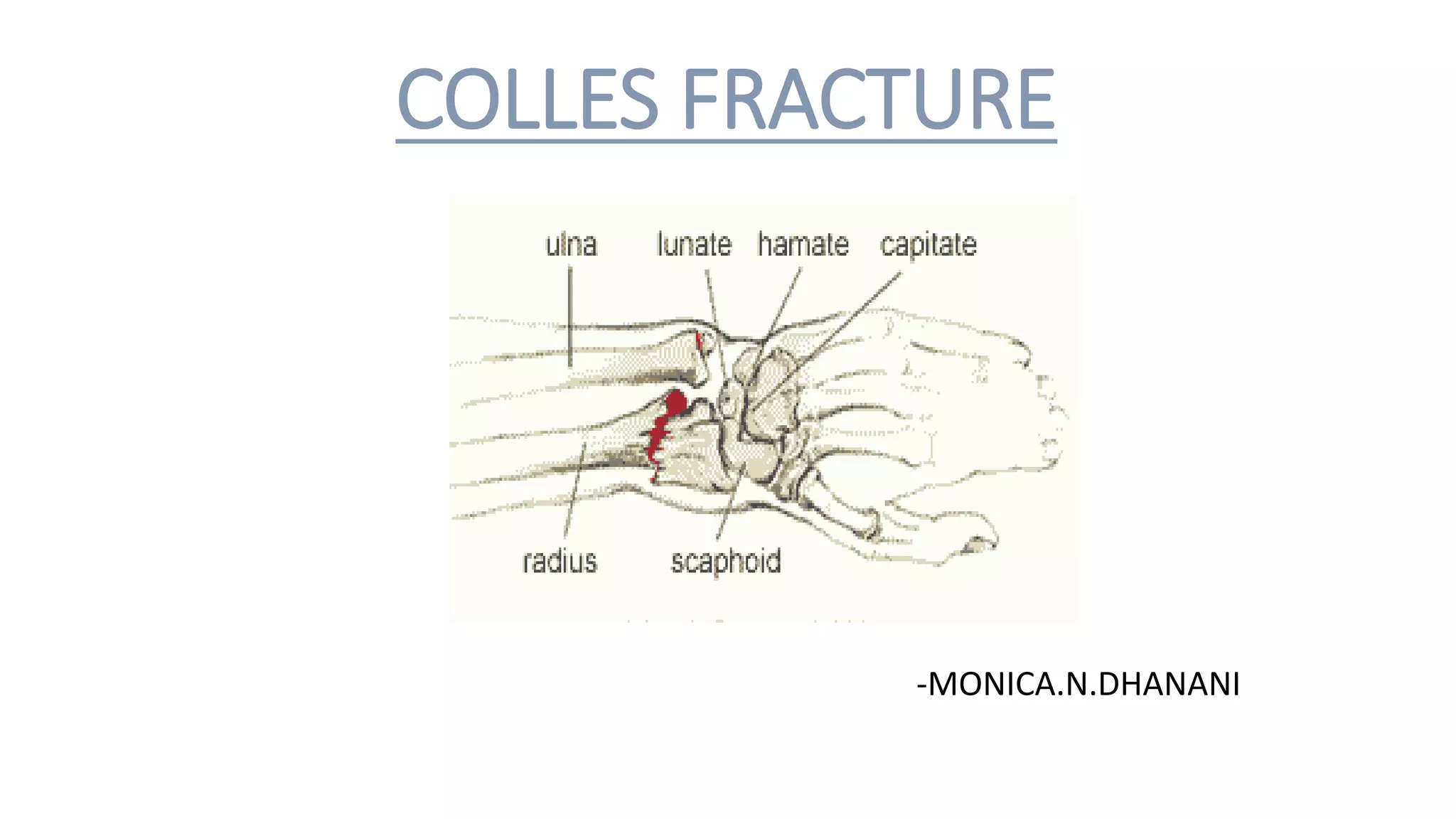
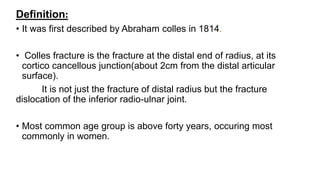
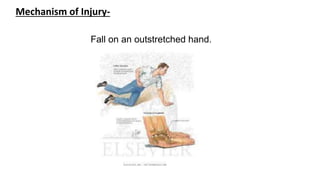
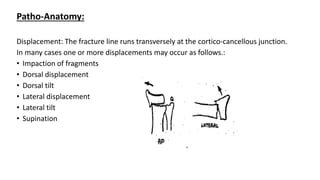
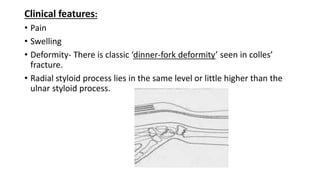
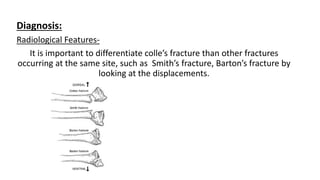
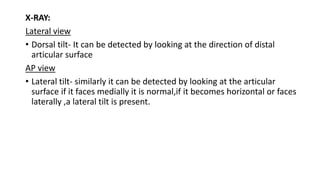
Colles' fracture is a fracture of the distal radius near the wrist. It often results in dorsal displacement of the distal fragment and occurs most commonly in women over 40 from falls on an outstretched hand. Clinical features include pain, swelling, and the classic "dinner fork deformity". Treatment depends on the degree of displacement, with undisplaced fractures treated conservatively in a cast and displaced fractures requiring manipulative closed reduction and casting or open surgical fixation with plates. Complications can include joint stiffness, malunion, subluxation, and nerve damage if not properly treated.


















































![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)




























