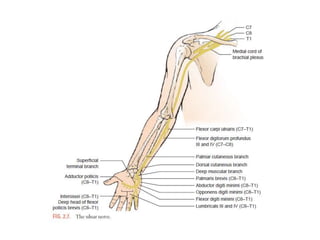
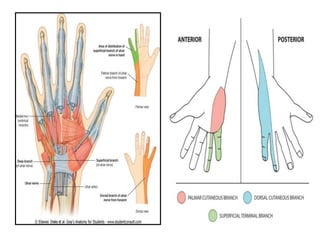
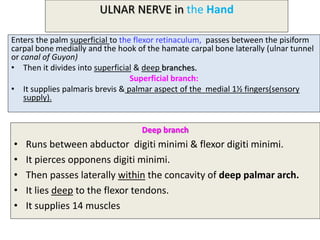
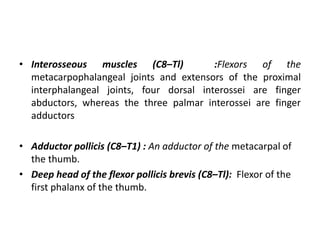
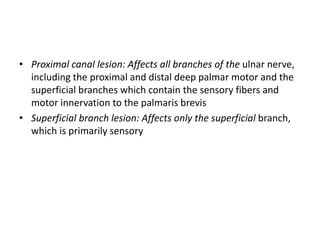
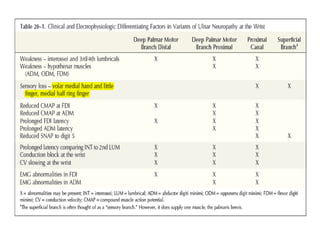
The ulnar nerve originates from the medial cord of the brachial plexus. It runs down the arm and enters the forearm between the two heads of the flexor carpi ulnaris muscle. In the hand, it passes through the ulnar tunnel, dividing into superficial and deep branches that provide sensory and motor innervation to portions of the fourth and fifth fingers. Lesions of the ulnar nerve can occur at different locations, with varying effects depending on whether the nerve is damaged proximally in the arm, at the elbow, in the forearm, or distally in the hand or wrist.
























































































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)




















