Downloaded 720 times
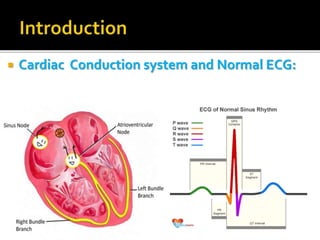
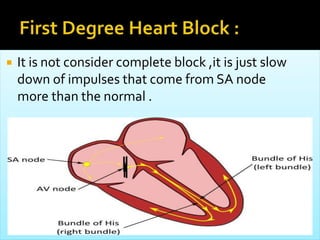
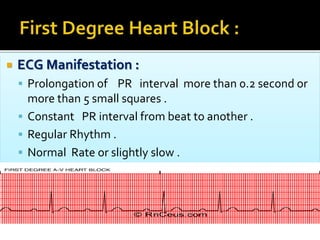
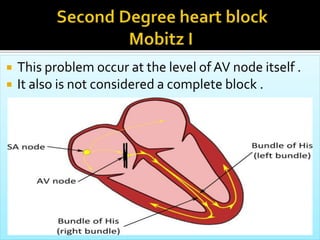
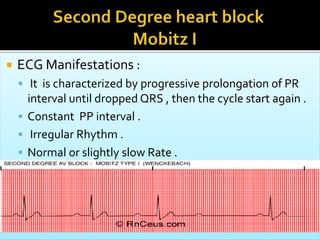
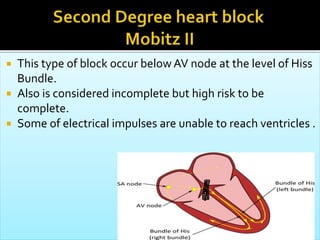
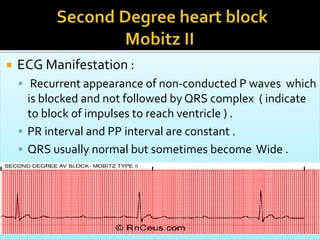
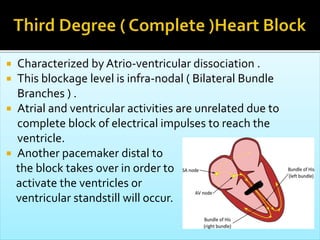
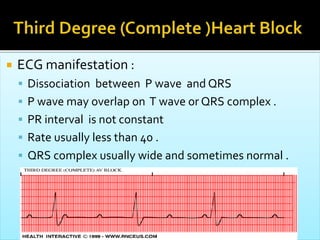


Atrioventricular heart block occurs when electrical signals between the atria and ventricles are interrupted or delayed. There are three types - first degree causes a prolonged PR interval, second degree is intermittent conduction with Mobitz types I and II, and third degree is complete block. Causes include myocardial infarction, medications, infections, degeneration. Symptoms range from none in first degree to bradycardia, hypotension, syncope in higher degrees. Treatment depends on symptoms but may include medication changes, temporary pacing, and permanent pacemaker for chronic cases.





























![ECG & Heart block [doctors online]](https://cdn.slidesharecdn.com/ss_thumbnails/ecgheartblockdoctorsonline-131111054313-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)










![Shadechapter12.ppt [read only]](https://cdn.slidesharecdn.com/ss_thumbnails/shadechapter12-150421103821-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







