Downloaded 84 times
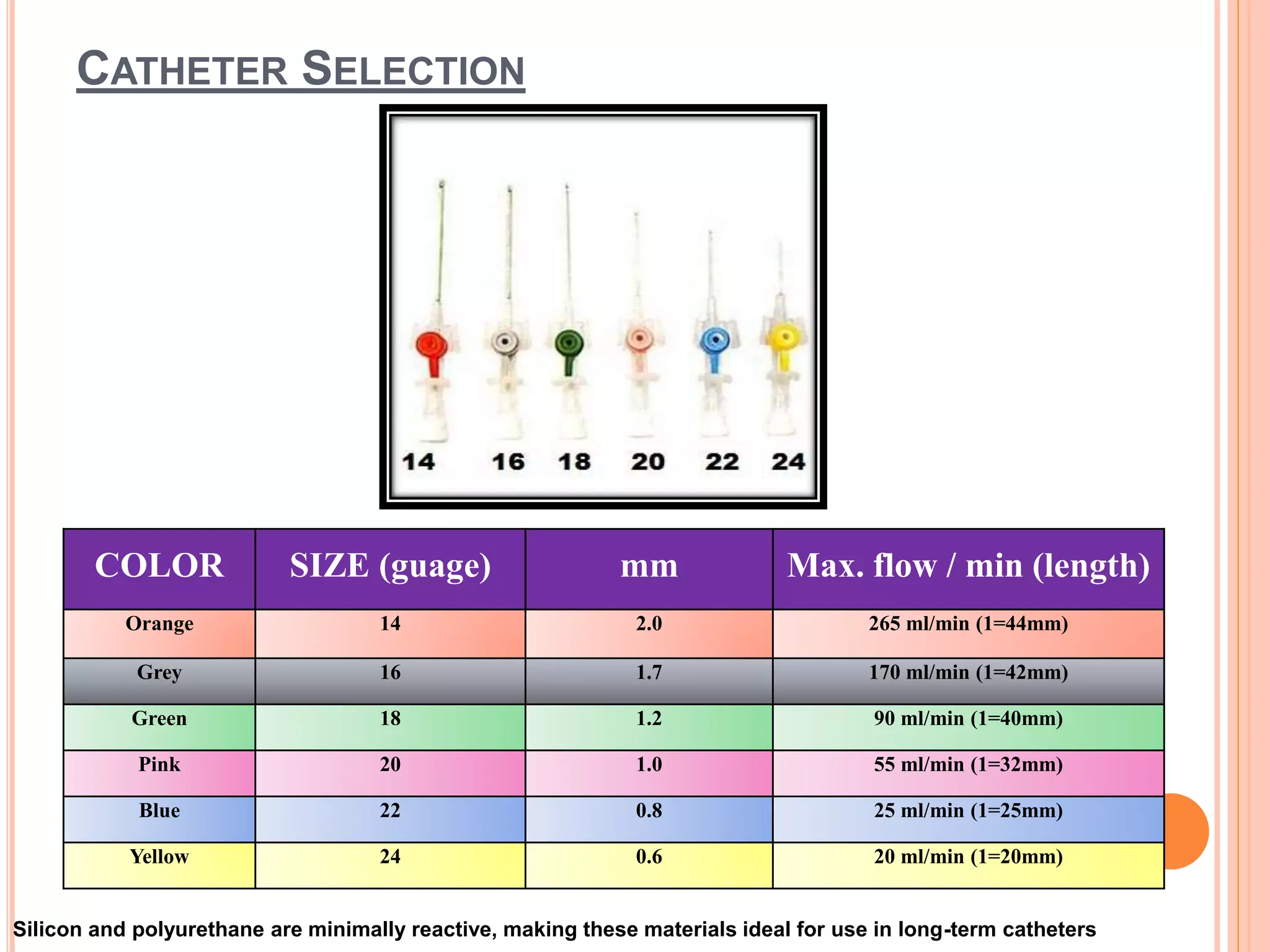

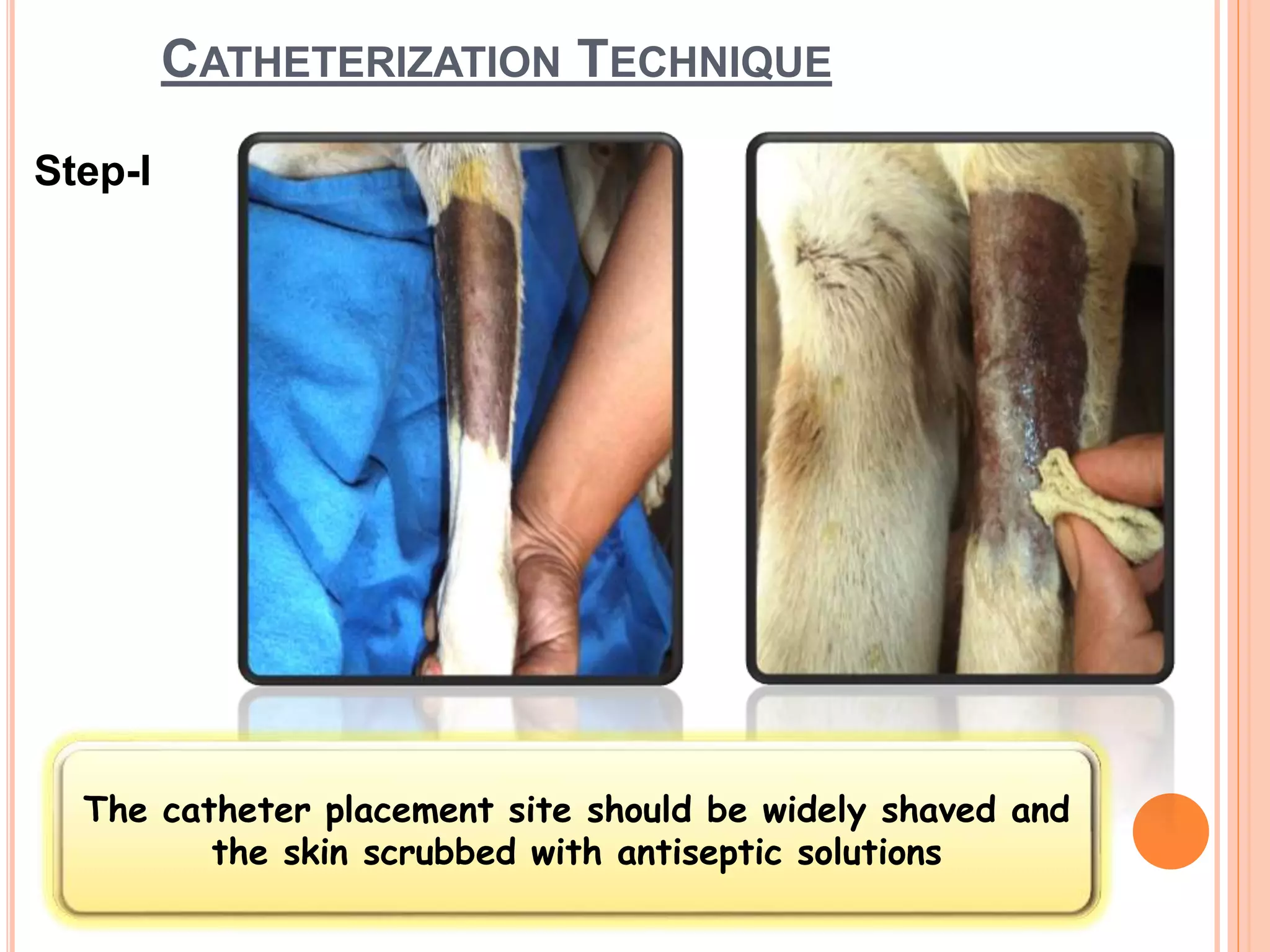
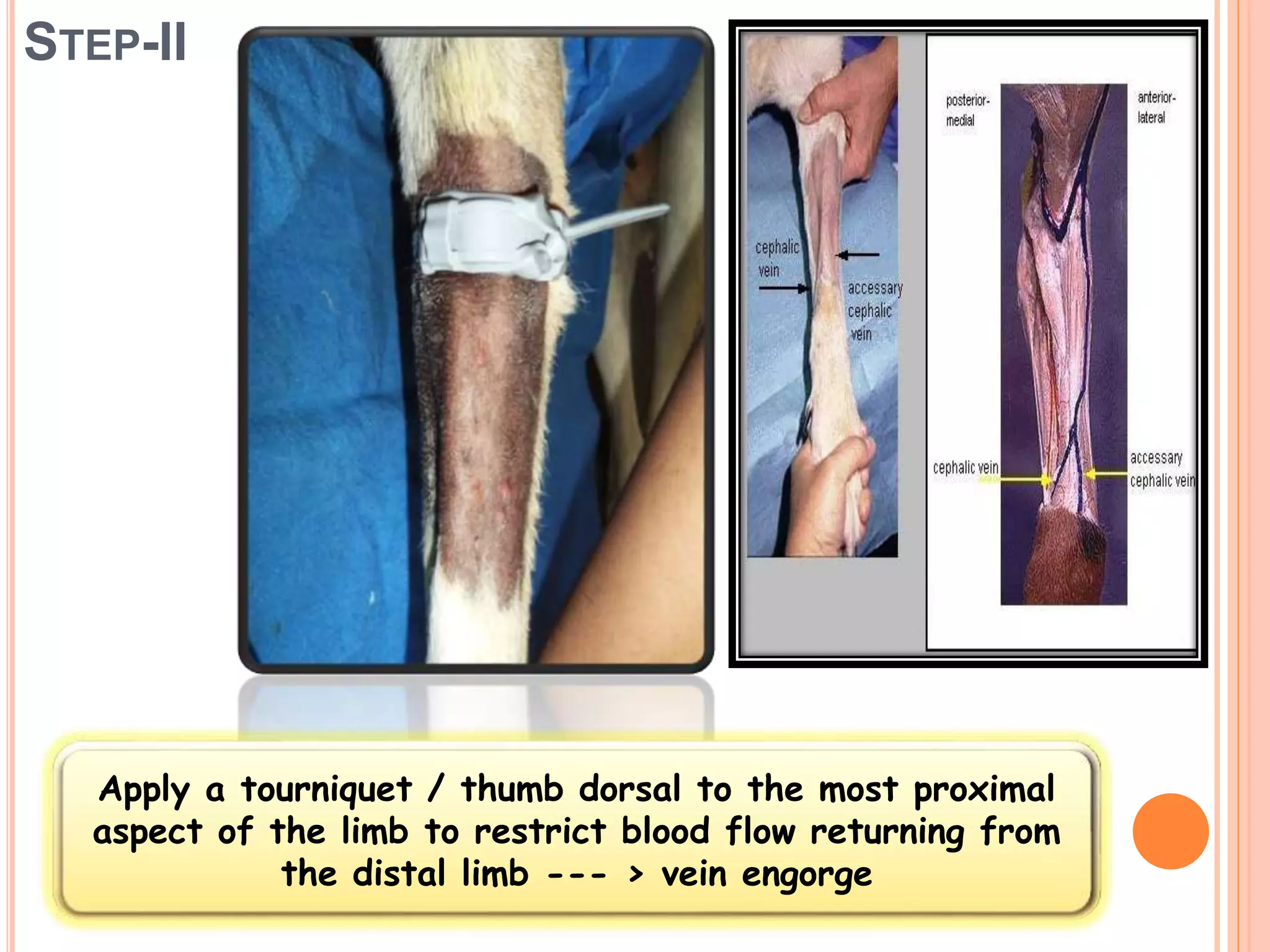
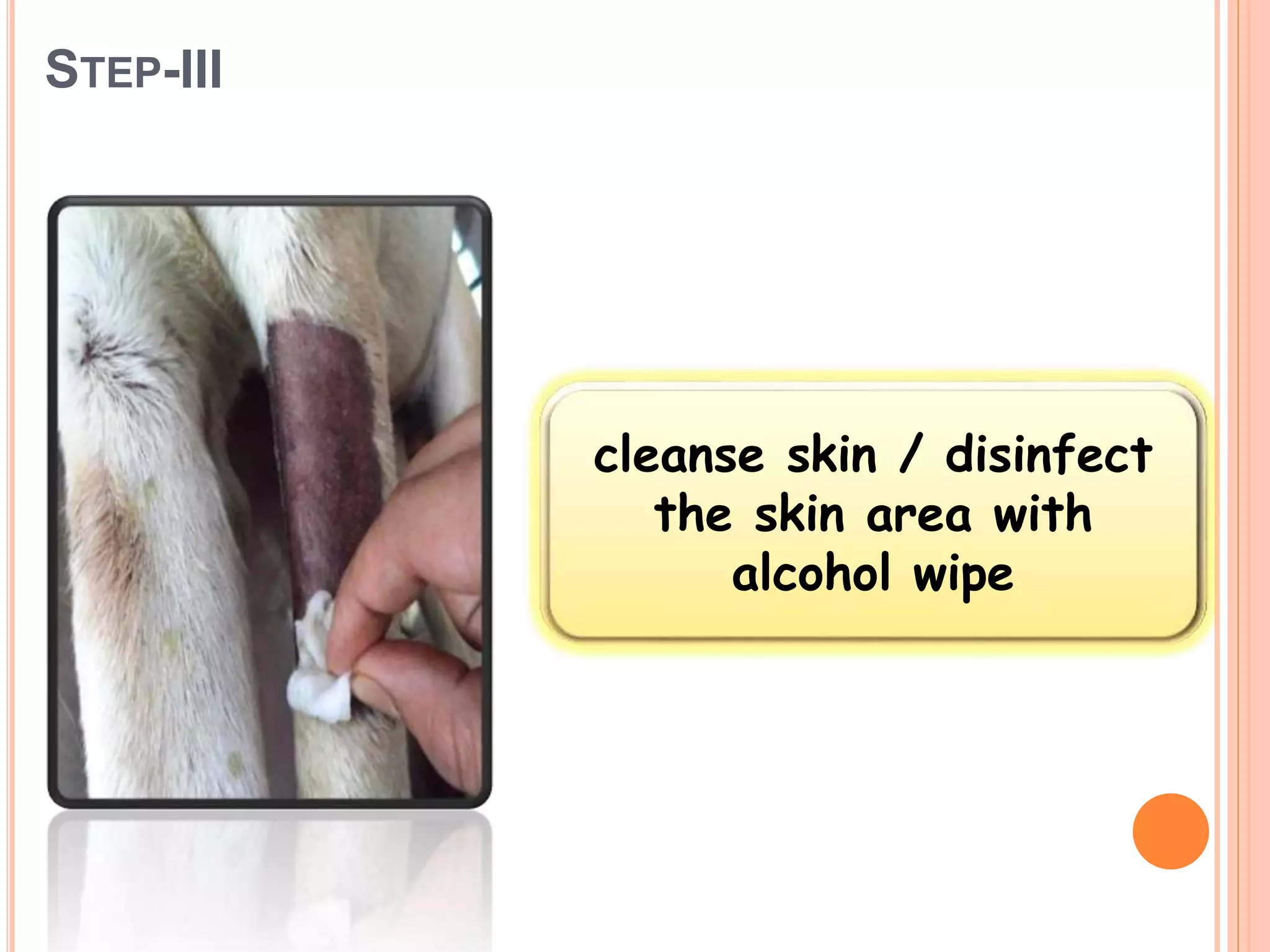









1. The document discusses the procedure for intravenous catheterization and taping. It describes selecting an appropriate catheter, preparing the skin, inserting the catheter into a vein, securing it, and caring for the catheter site. 2. Key steps in the procedure include shaving and disinfecting the skin, inserting the needle at a 30-40 degree angle to access the vein, securing the catheter with tape to prevent dislodgement, and flushing it with saline to maintain patency. 3. The catheter should be secured carefully and the site inspected regularly for signs of phlebitis. Peripheral catheters should be resited every 48-72 hours to reduce risks of infection and phlebit











































































































