This document provides information on intravenous cannulation including:
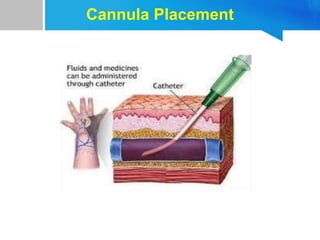
1) Definitions of IV cannulation and the different types of cannulae and their gauges and flow rates.
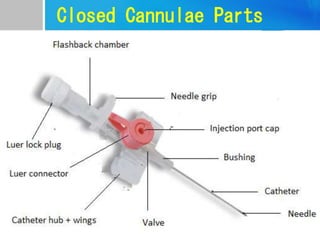
2) The parts of closed cannulae and different types of fixators.
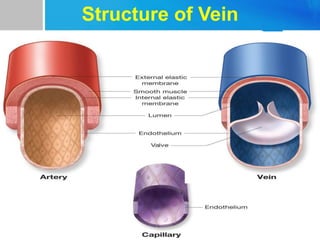
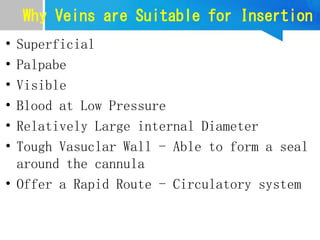
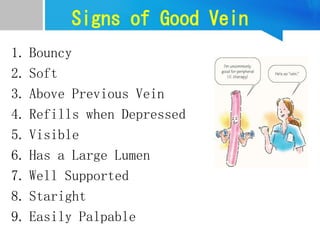
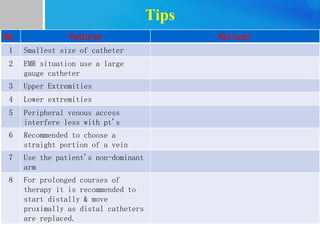
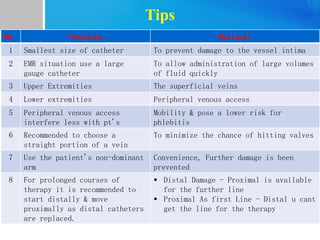
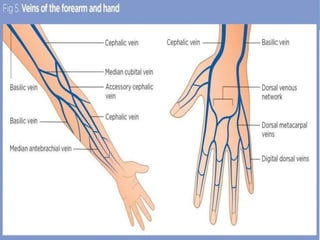
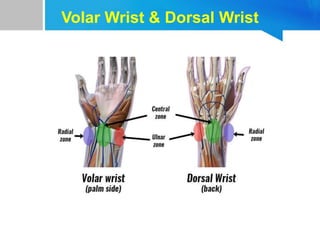
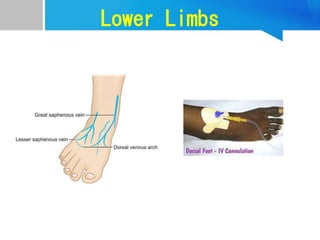
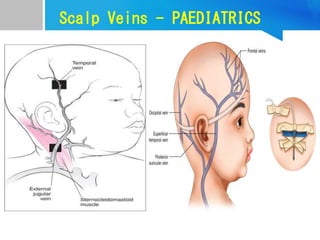
3) Tips for selecting appropriate veins and sites on patients and contraindications.
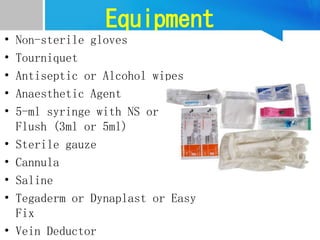
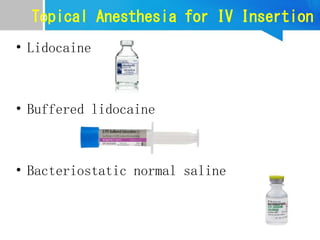
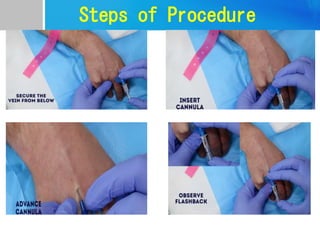
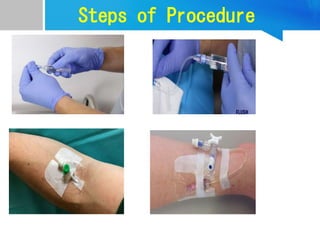
4) Steps for performing IV cannulation including equipment, preparation, technique, complications and documentation.