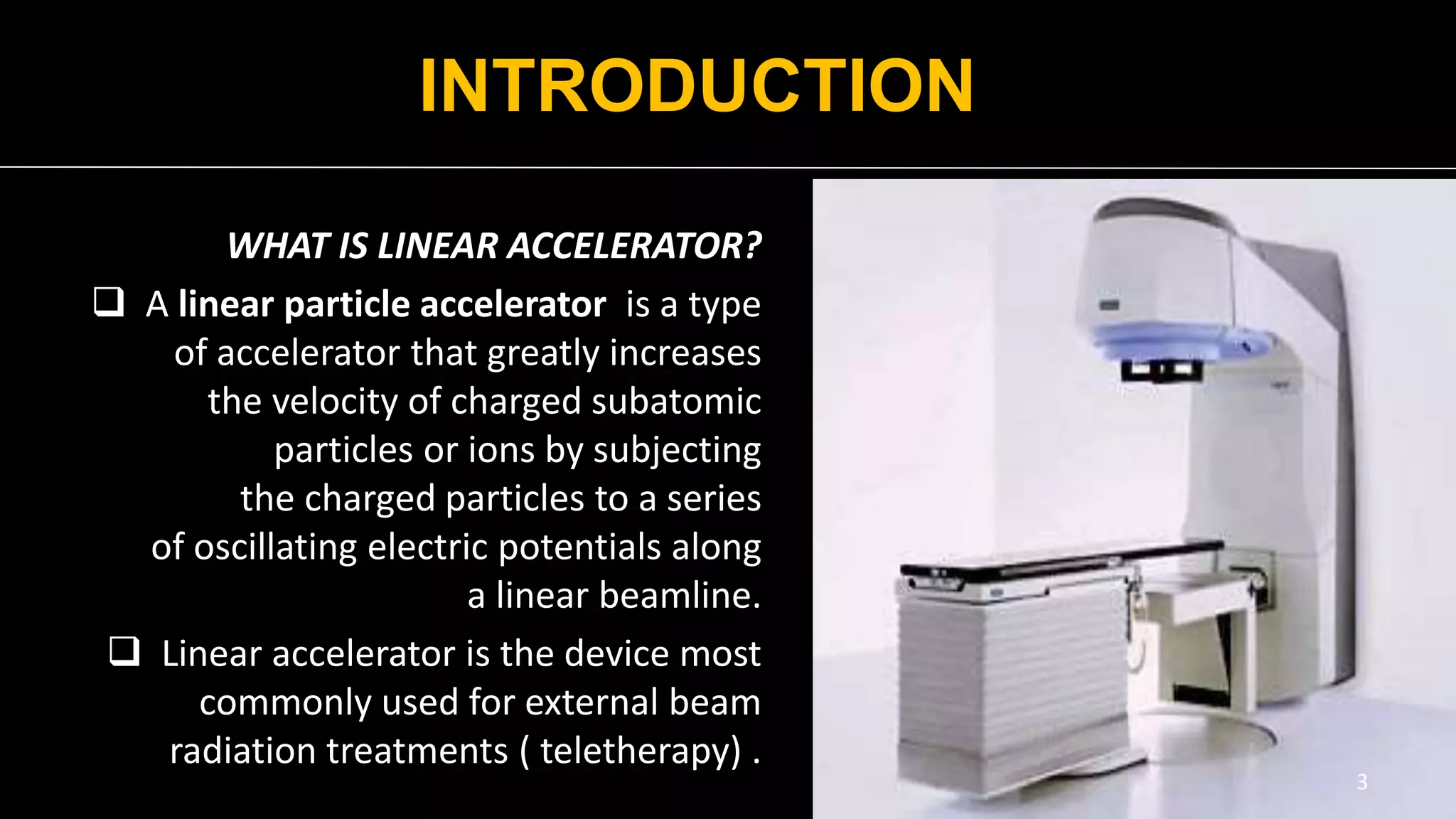
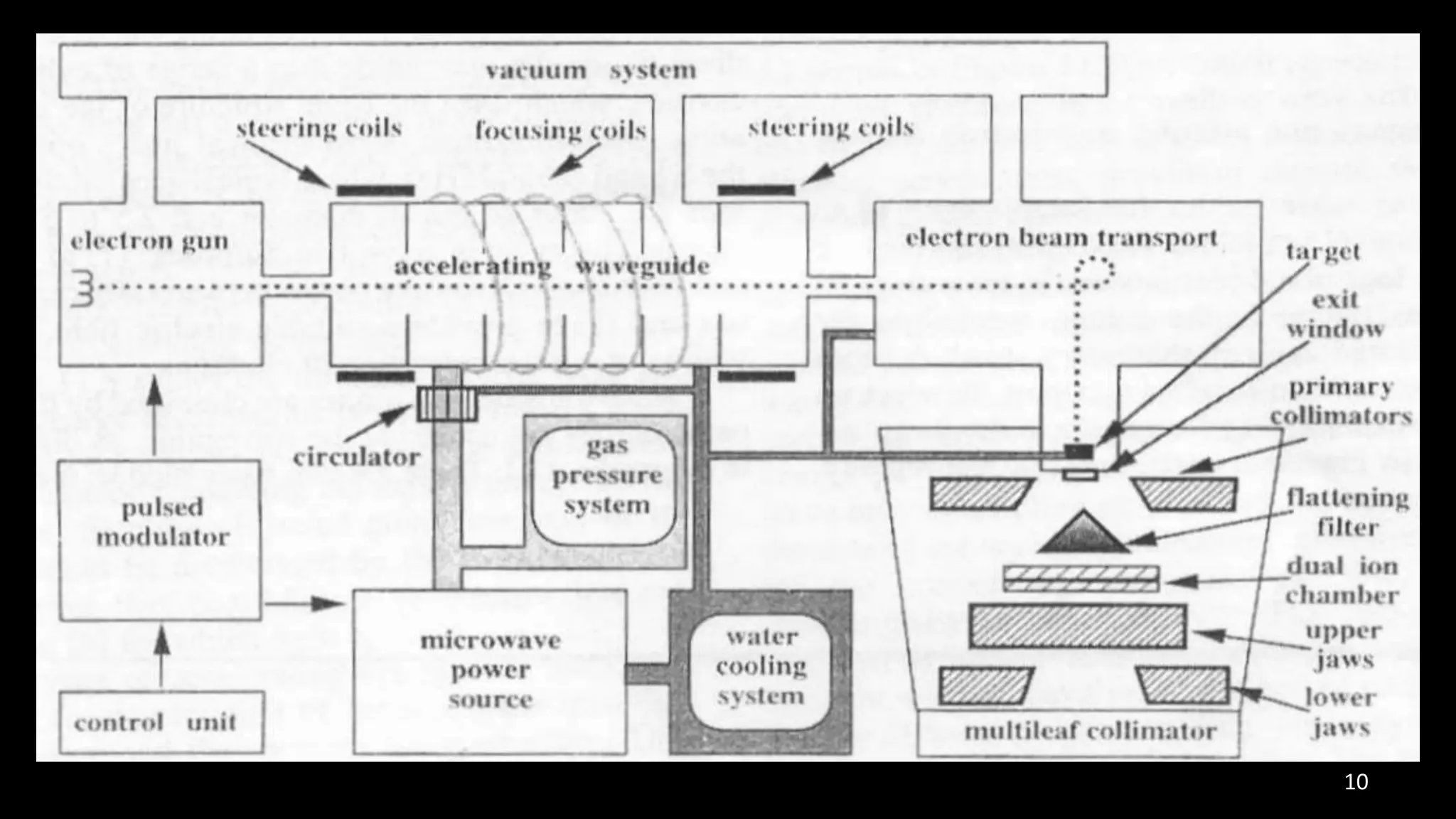
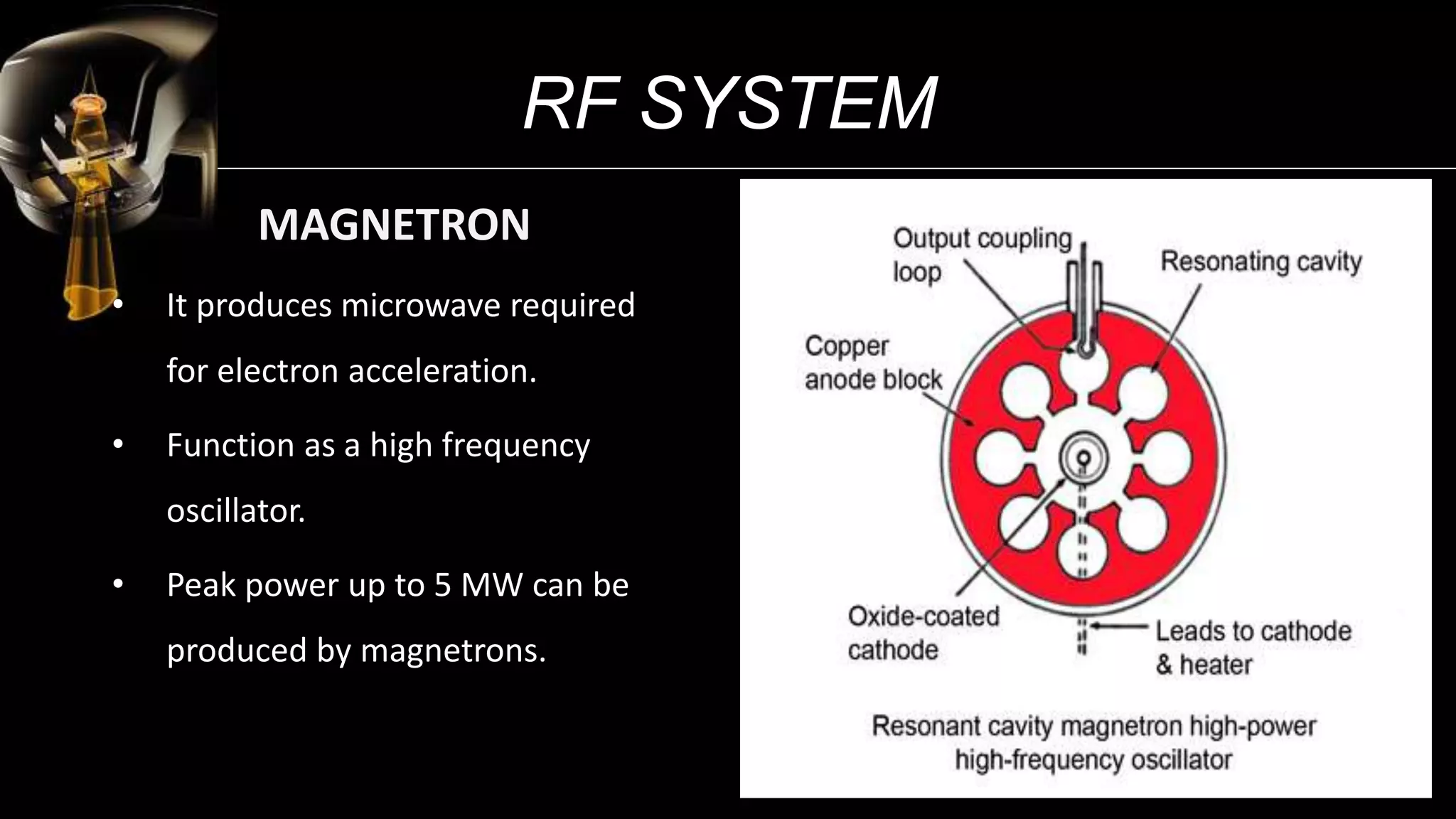
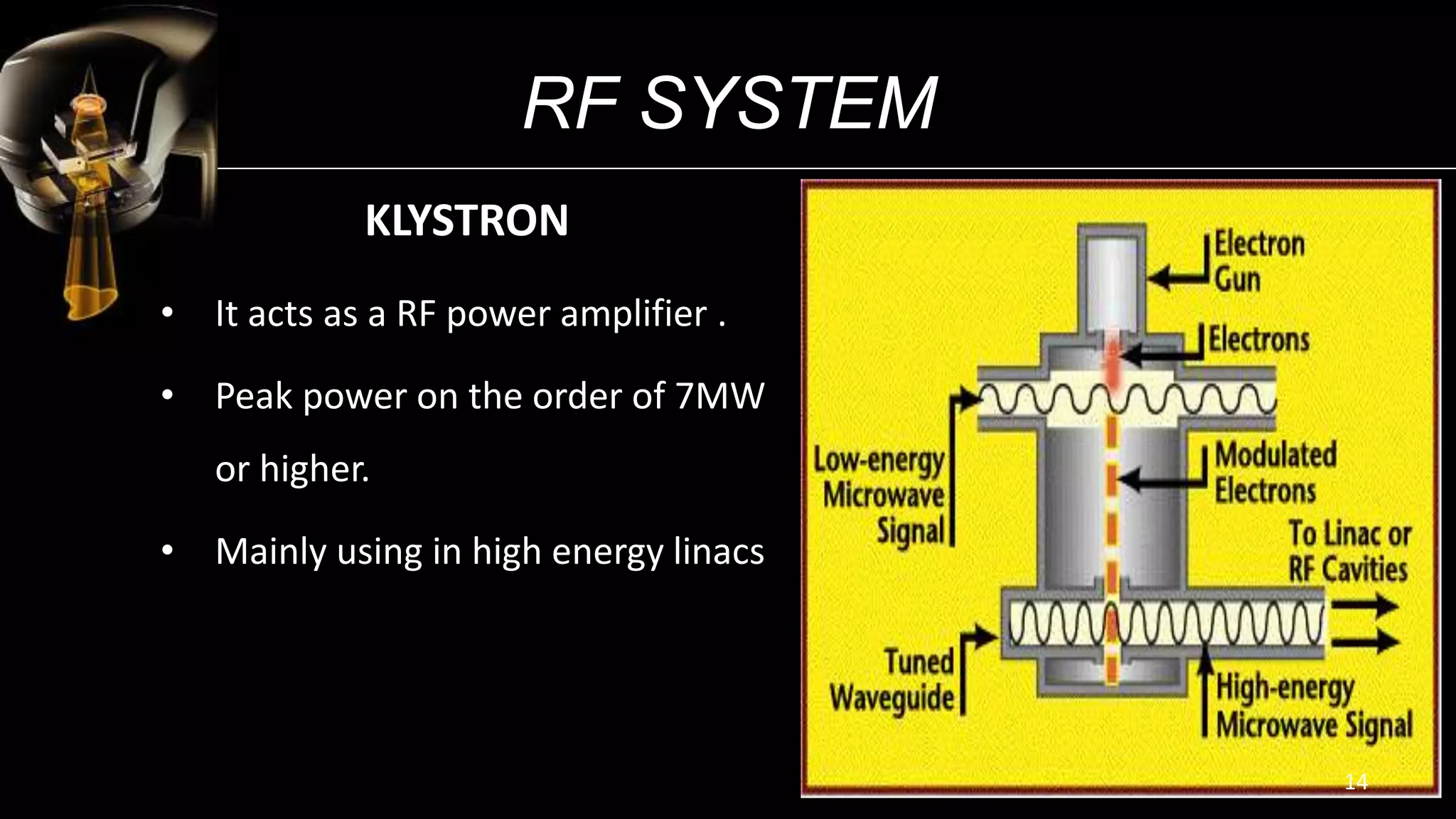
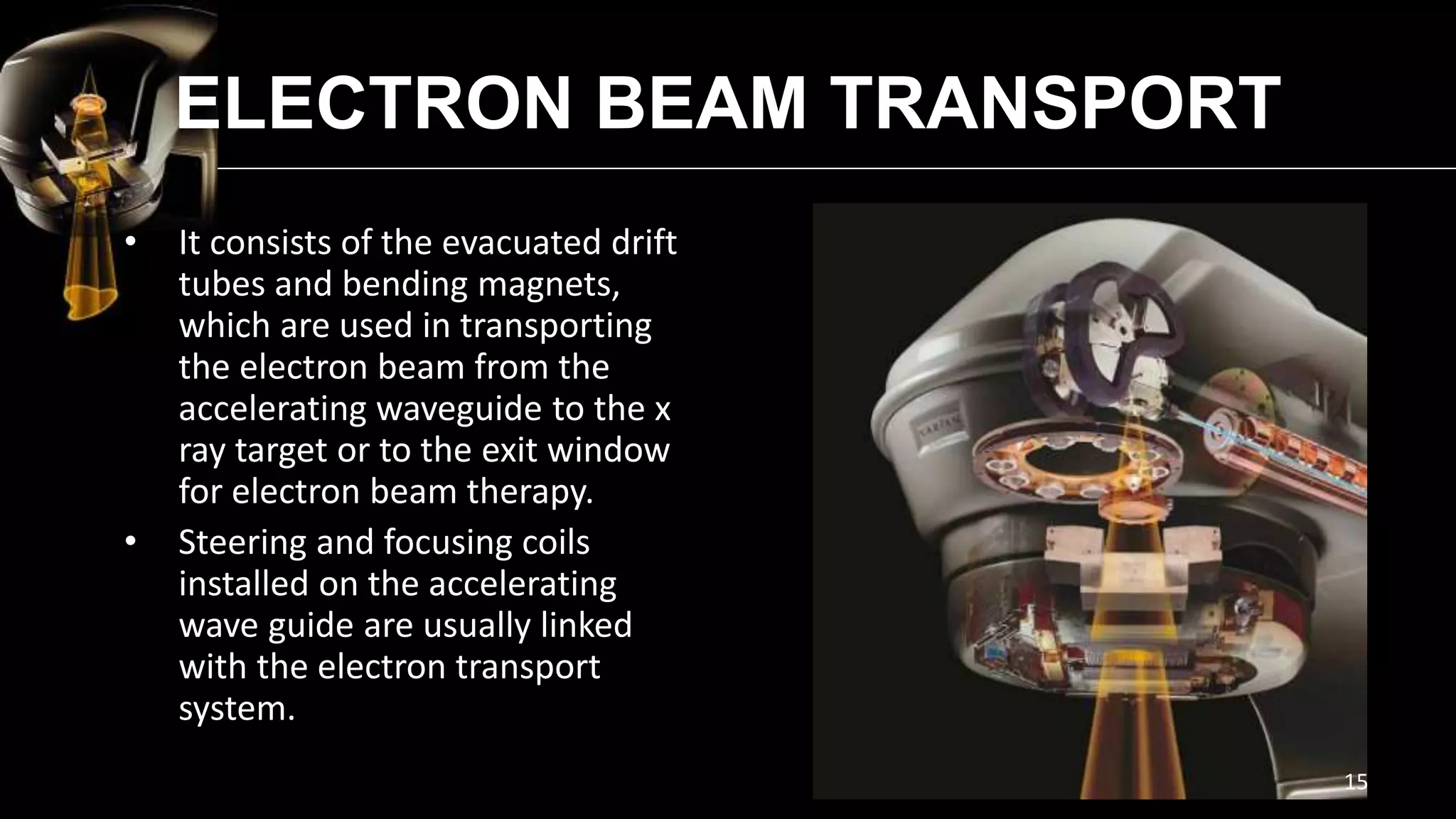
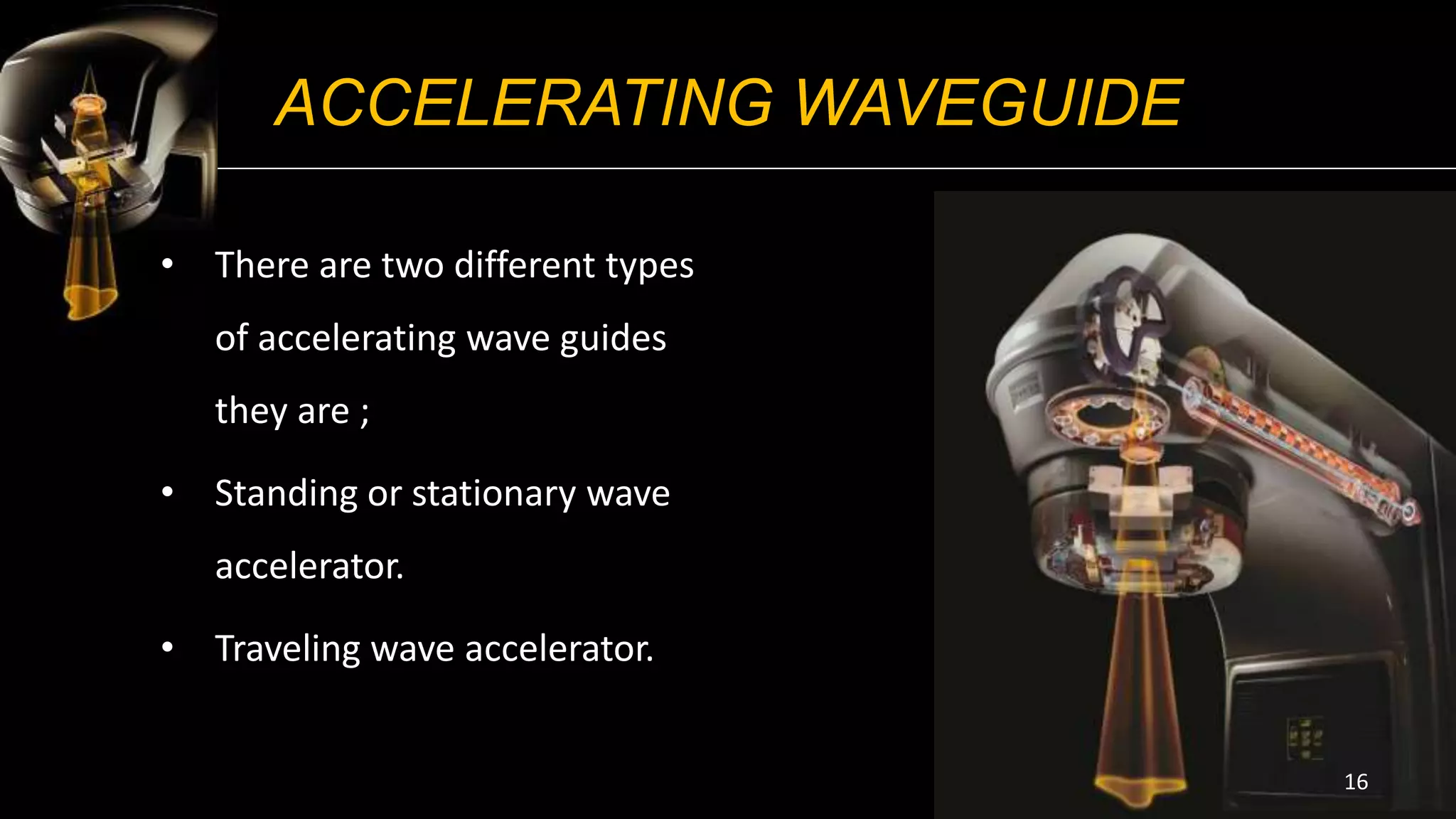
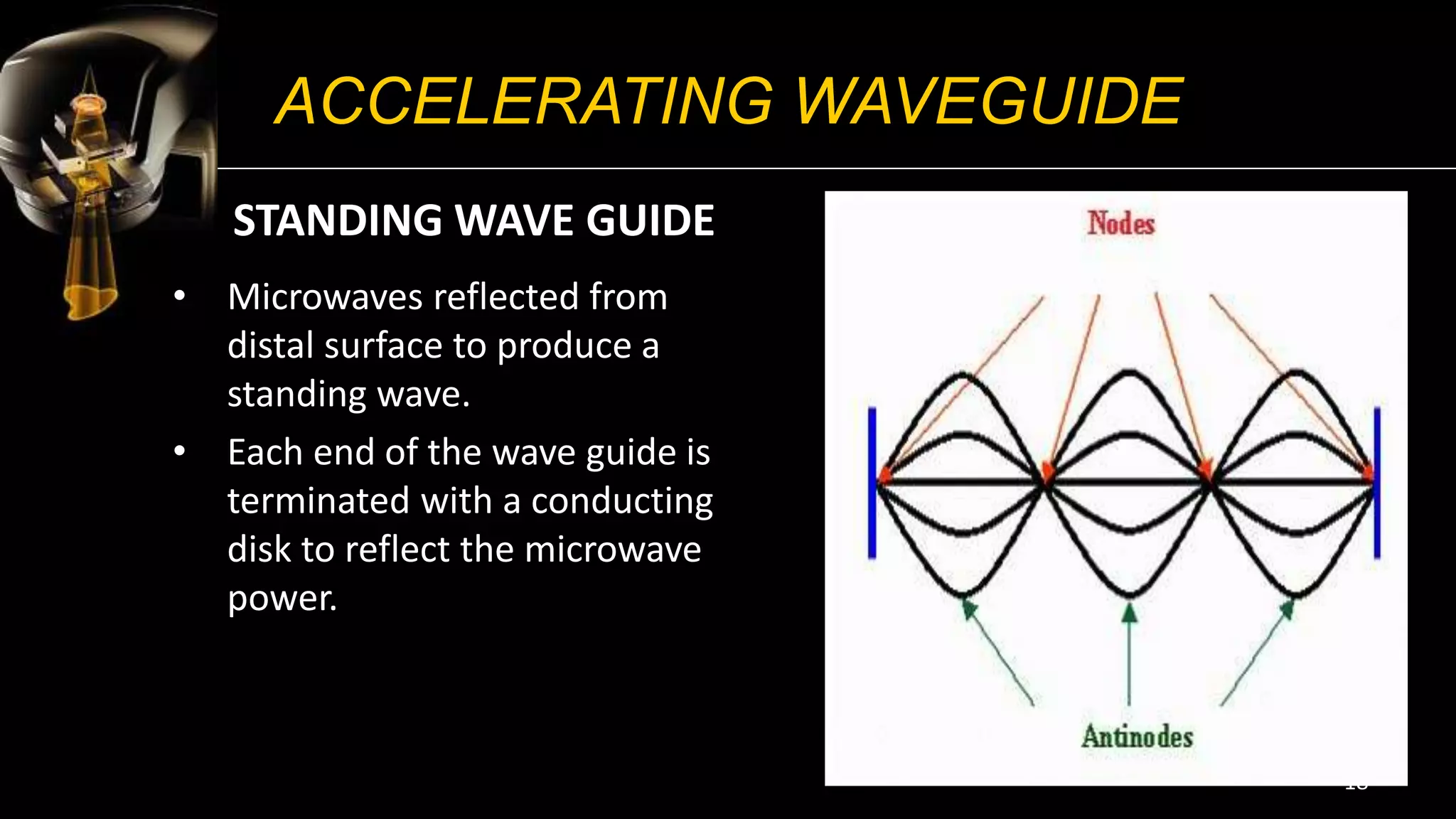
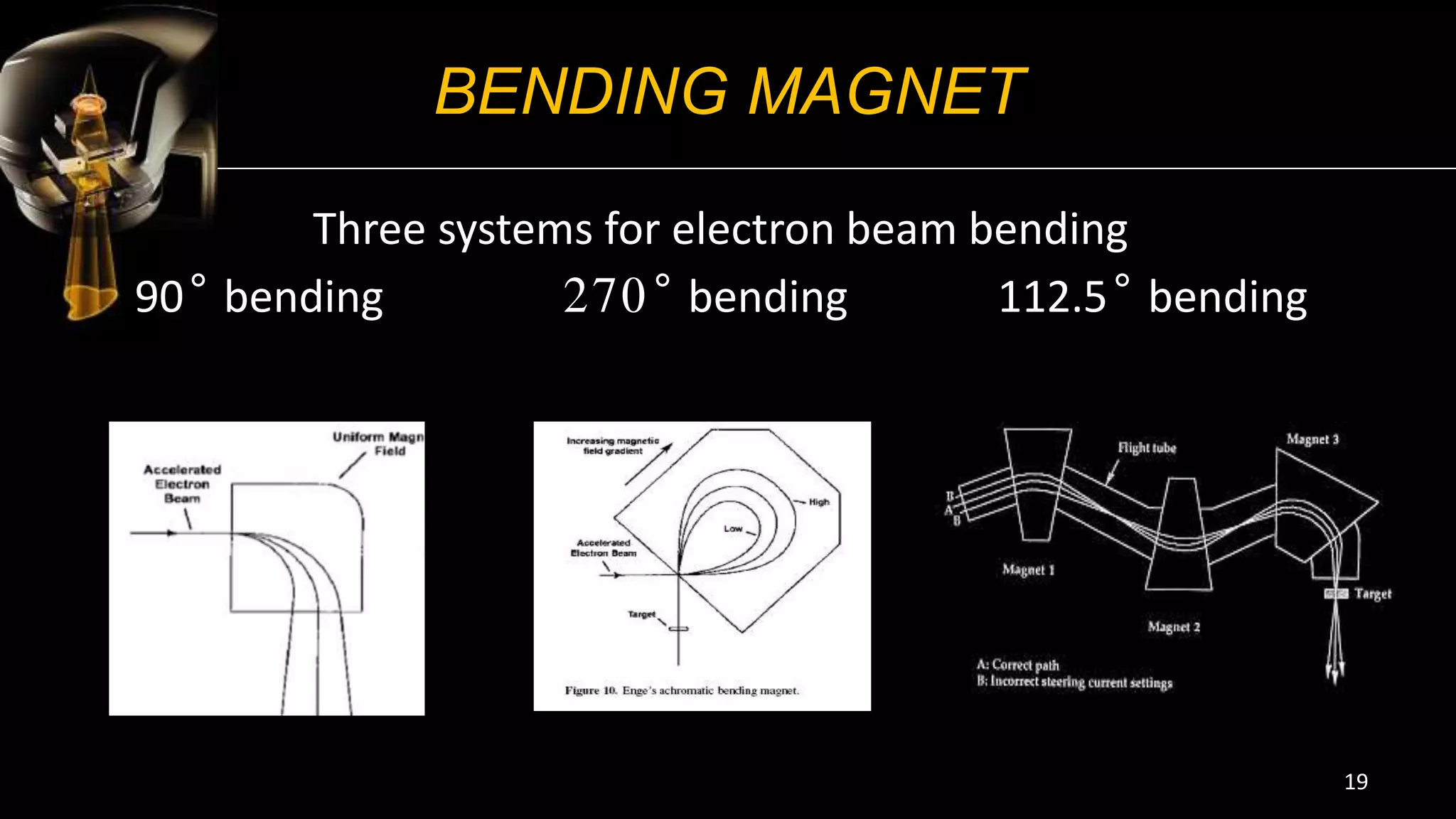
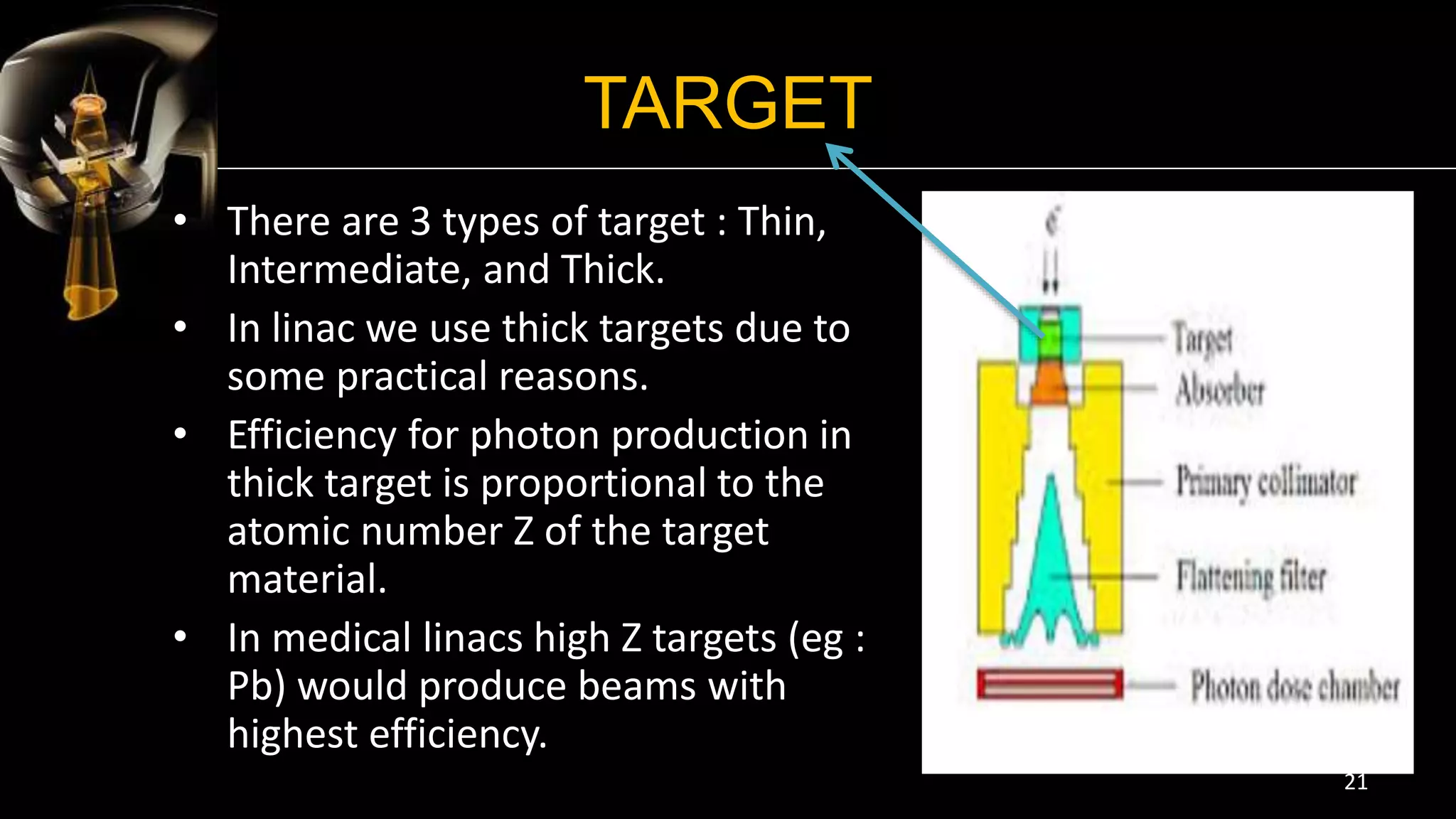
Linear accelerators use microwave technology to accelerate electrons, which are then collided with a heavy metal target to produce high-energy photons. The photons are shaped and directed to the patient's tumor. The main components of a linear accelerator include the injection system to produce electrons, the RF system to accelerate the electrons, auxiliary systems, beam transport to deliver electrons to the target, and beam collimation and monitoring systems to shape and measure the photon beam. Linear accelerators have gone through several generations with improvements like higher photon energies, computer control, dynamic wedges, and intensity modulated radiation therapy.





































































![[equipment iv] linacc](https://cdn.slidesharecdn.com/ss_thumbnails/sbmeequipmentivlinac-200915164740-thumbnail.jpg?width=640&height=640&fit=bounds)



















