Downloaded 24 times
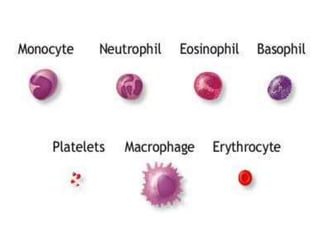
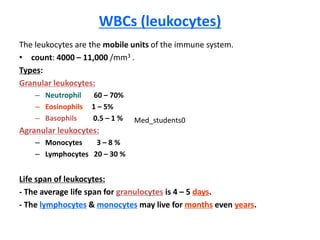
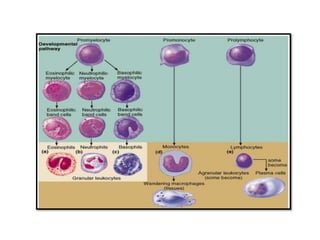
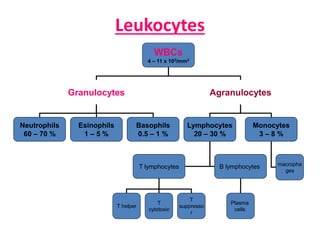
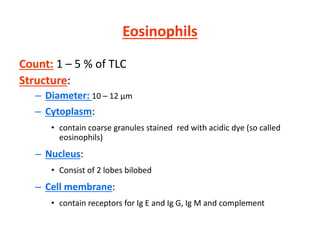

White blood cells (WBCs) or leukocytes are the mobile units of the immune system that help protect the body from infection and disease. There are two main types of WBCs: granulocytes which have granules in their cytoplasm and include neutrophils, eosinophils, and basophils; and agranulocytes which do not have granules and include lymphocytes and monocytes. Each type of WBC has a specific function such as phagocytosis, antibody production, or regulation of the immune response. Together, WBCs provide a powerful defense mechanism against infections, tumors, and toxins.
![White blood cells [wbc]](https://cdn.slidesharecdn.com/ss_thumbnails/whitebloodcellswbc-180530054405-thumbnail.jpg?width=640&height=640&fit=bounds)






















































































