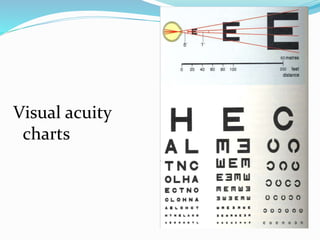
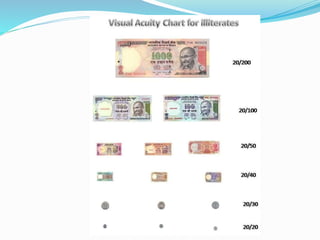
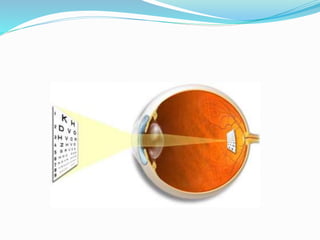

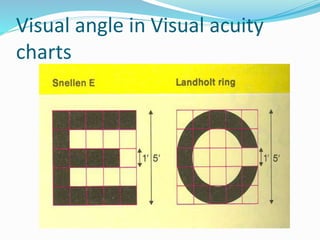

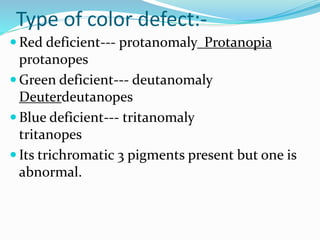
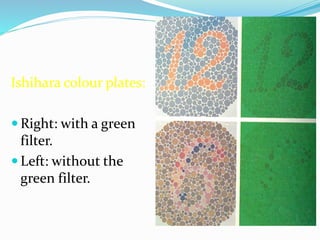
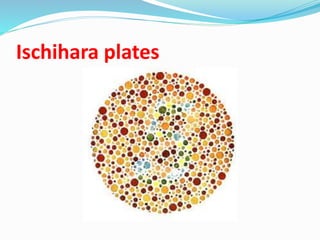
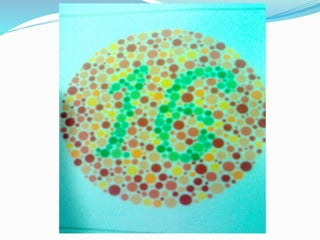

Visual acuity is measured using charts with letters of decreasing size, with the Snellen chart being most common. It represents the sharpness of vision and is recorded using a fraction where the numerator is the test distance in feet and the denominator is the smallest line read on the chart. Additional tests include visual fields, color vision, and pinhole tests to determine if vision problems are due to refractive errors or other issues. Color vision is assessed using plates like Ishihara that people with normal color vision can interpret but those with defects cannot.











































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










