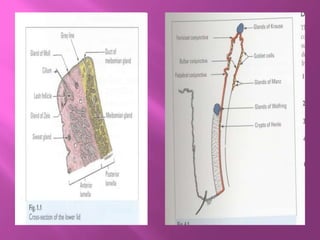

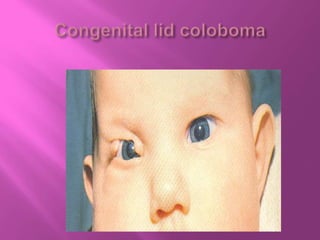
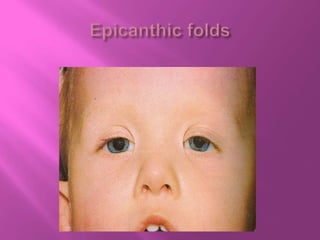












This document provides information about the anatomy and structures of the eyelids. It discusses the skin, muscle layers, tarsal plate, and palpebral conjunctiva that make up the eyelid. It describes the functions of the eyelids in protecting the eyes, distributing tears, lubricating the eyeball, and enabling emotional expressions. The document also briefly mentions several eyelid conditions like coloboma palpebral, distichiasis, and blepharophimosis.























































































