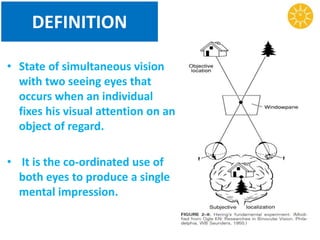
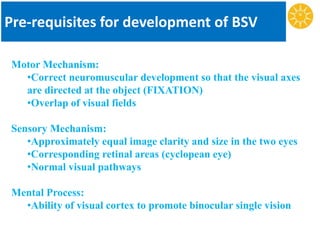
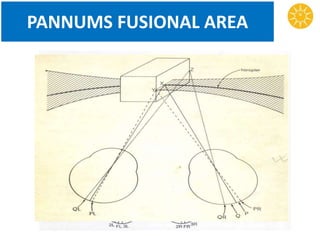
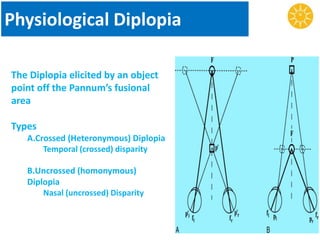
Binocular vision refers to the coordinated use of both eyes to produce a single mental impression. It develops through childhood as the visual and motor mechanisms mature. Theories of binocular vision aim to explain how a single visual percept is formed from two retinal images. Key components include retinal correspondence, the horopter curve, and Panum's fusional area. Abnormalities can disrupt binocular vision and cause issues like diplopia or suppression. Clinical tests evaluate retinal correspondence, stereopsis, and fusional abilities to assess binocular function.


![PERCEPTION OF DEPTH
• Perception of distance of objects from each
other or from the observer.
• Several clues contribute-
A] BINOCULAR CLUE: Stereopsis.
B] MONO OCULAR CLUES:](https://image.slidesharecdn.com/binocularvision-151009131006-lva1-app6892/85/Binocular-vision-30-320.jpg)