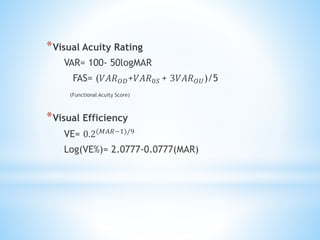
This document summarizes visual acuity testing and measurement. It discusses various tests used to measure visual acuity including Snellen charts, Landolt rings, Tumbling E charts, and picture charts. It explains how visual acuity is recorded and interpreted using Snellen fractions, decimals, and logarithm of the minimum angle of resolution. The document also discusses objective tests of visual acuity for infants and children such as preferential looking tests, optokinetic nystagmus tests, and grating acuity tests.