Downloaded 594 times
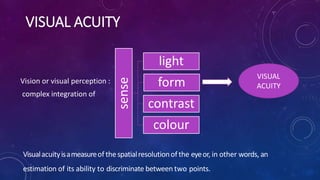
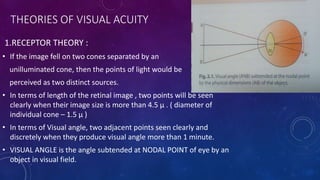
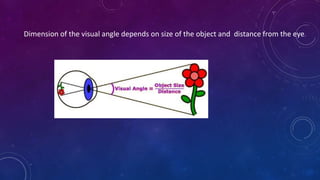

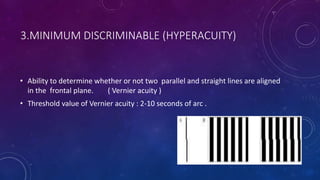
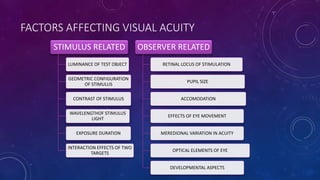
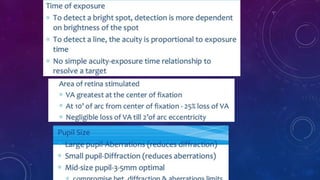
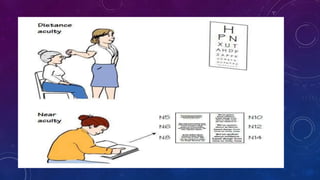
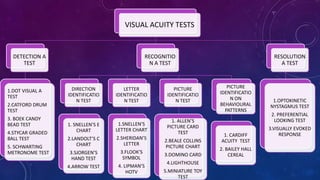

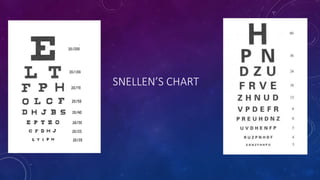

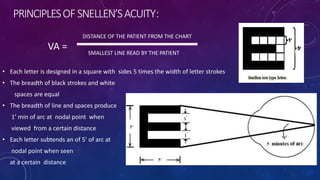
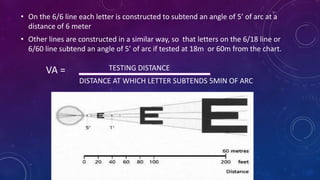




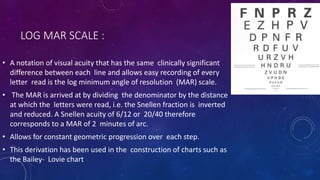





Visual acuity is a measure of the eye's ability to see fine detail and discriminate between objects. It is assessed using charts with letters, symbols, or pictures of decreasing size. The Snellen chart is commonly used, with visual acuity recorded as the distance at which a person can see a symbol subtending an angle of 5 minutes of arc. Other methods include the Landolt C chart and LogMAR chart. Visual acuity depends on factors like stimulus characteristics, retinal location stimulated, and optical elements of the eye. It provides information on visual function, refractive status, and outcomes of treatments.














































































