
































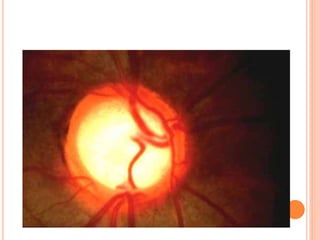
![PRIMARY ANGLE CLOSURE GLAUCOMA :
Definition :It’s a condition in which IOP increase
because the outflow of aqueous humor from the
anterior chamber is mechanically impaired by
contact of the iris with the trabecular drainage
meshwork and peripheral cornea ----- decrease angle
of A.C .
Females are more affected [F:M---3:1], Age incidence
40 – 45 Y.
Usually bilateral {2nd eye involved after 1 year}.
Predisposing factors:
Nervous anxious persons . Small eyeball { in
hyperopies }.
Family history . Females more affected .
Age: with increase age lens become large ---- A.C get
shallower and it s angle narrower .
Thick iris --- may narrow A.C angle .](https://image.slidesharecdn.com/glaucoma-190622093805/85/Glaucoma-38-320.jpg)

















![ACUTE STAGE {EMERGENCY CASE }:
I.V mannitol 20% {hypertonic agent }.
Oral glycerol {glycerine }1 ml / kg .Both act as hypertonic
or osmotic agents --- making blood hypertonic ---drawing fluid
form the eye --- decrease IOP.
Isosorbide orally for diabetic patient & urea 1-2gm/kg
Pilocarpine drops 4% every 5 min (drop every minute).
Pilocarpine constricts the pupil ---- pulls the iris away from
{posteriorly}trabecular meshwork ---- reestablished aqueous
outflow .
Acetazolamide 250 – 500 mg IV or orally
[Diamox].Acetazolamide {carbonic anhydrase inhibitor }---
decrease production of aqueous .
Beta blockers { timolol } locally 0.25 -0.5 % ---- decrease
aqueous production .
Steroid-antibiotic e.d. for congestion
Analgesics and sedatives
When IOP is controlled ----give Pilocarpine 1% only .](https://image.slidesharecdn.com/glaucoma-190622093805/85/Glaucoma-60-320.jpg)




























































































Glaucoma is a disorder caused by increased intraocular pressure damaging the optic nerve. It has two main types - open angle glaucoma where the angle remains open, and angle closure glaucoma where the angle becomes narrow or closed. Angle closure glaucoma occurs when the iris blocks the drainage angle, commonly due to pupillary block or narrowing of the angle with age. It presents with sudden severe eye pain, blurred vision, headache, and eye redness. Gonioscopy is used to examine the angle structure and grade its width.






















































































