Download as PDF, PPTX






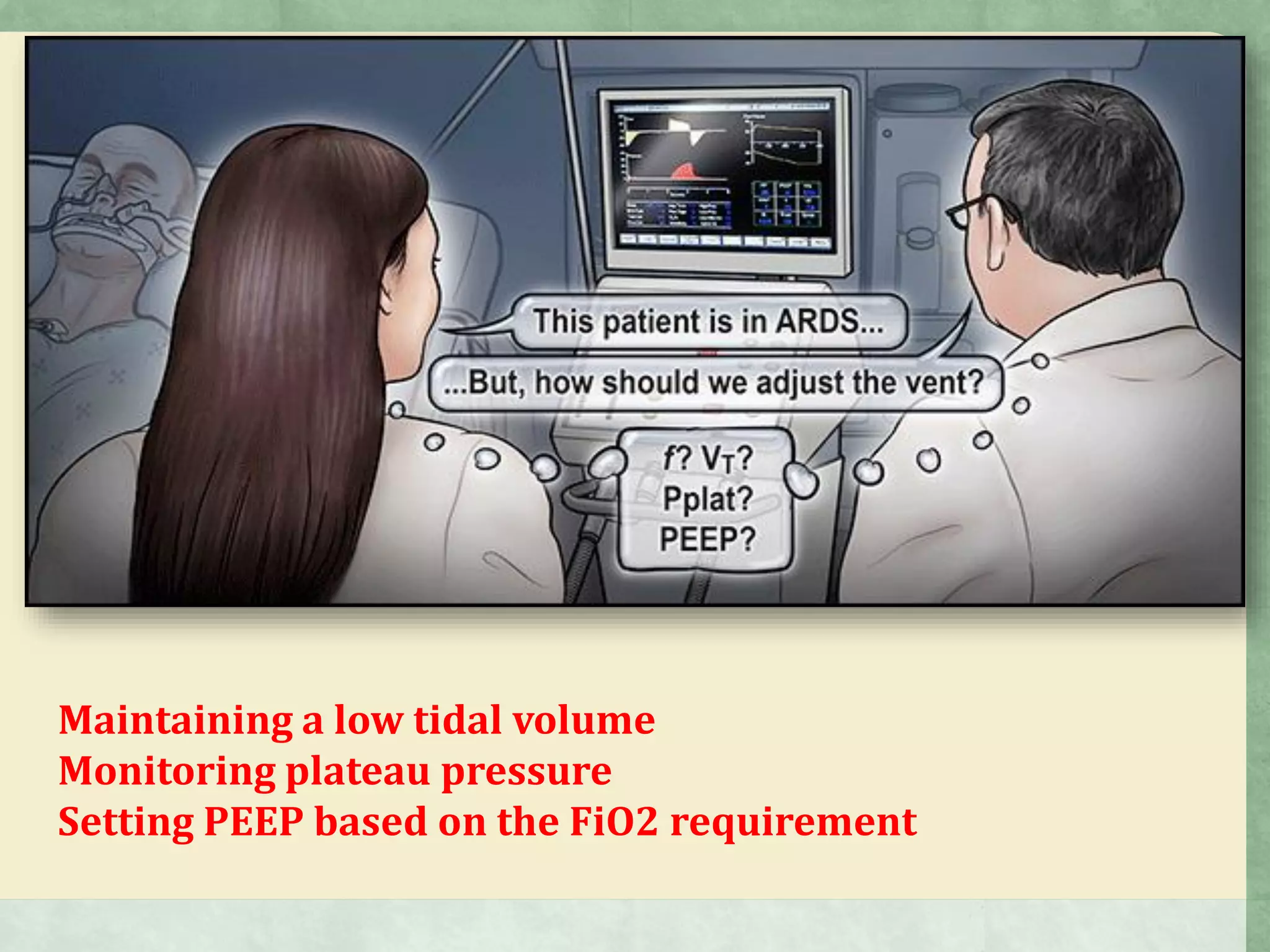

































































This document discusses various topics related to ARDS including definitions, causes, ventilator strategies, and treatments. It provides the American-European Consensus definition of ARDS which requires bilateral infiltrates, hypoxemia, and no evidence of cardiogenic pulmonary edema. Common causes of ARDS are also mentioned. Regarding ventilator management, low tidal volumes, appropriate PEEP levels based on oxygen needs, and maintaining low plateau pressures are emphasized. Additional strategies discussed include prone positioning, recruitment maneuvers, and neuromuscular blockade. While high frequency oscillatory ventilation and inhaled treatments were investigated, they did not show clear benefits.














































































