Download as PDF, PPTX
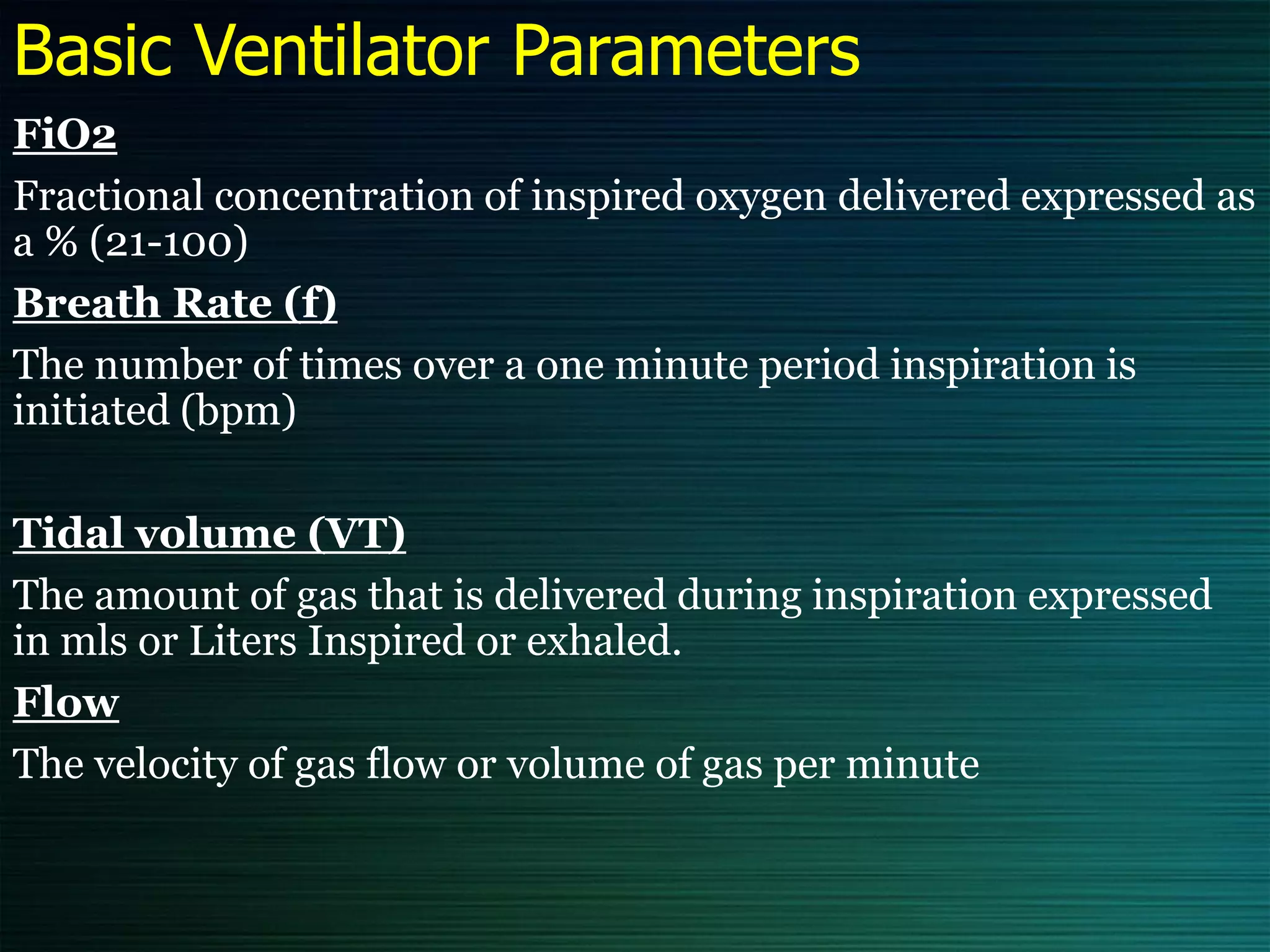
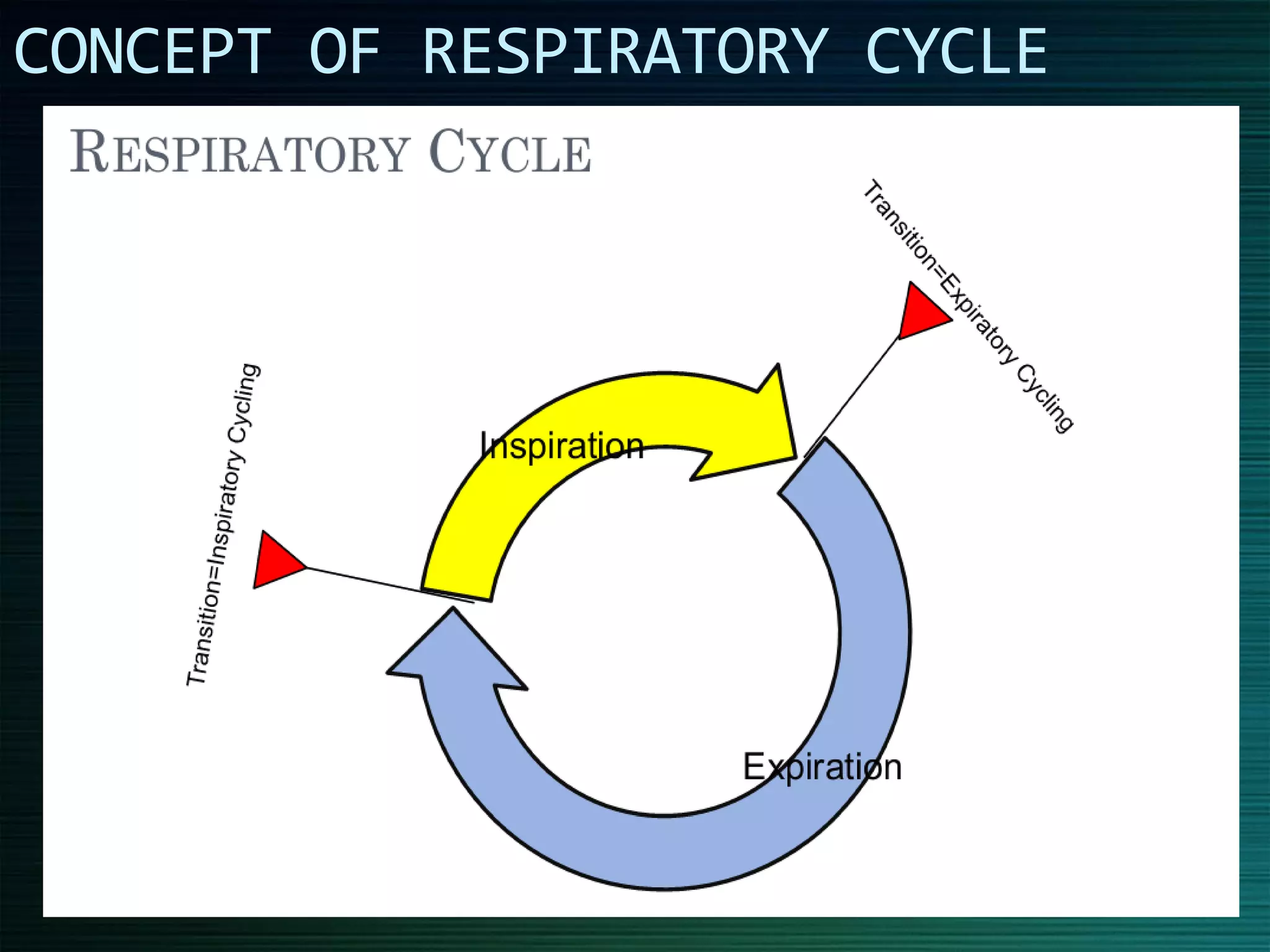
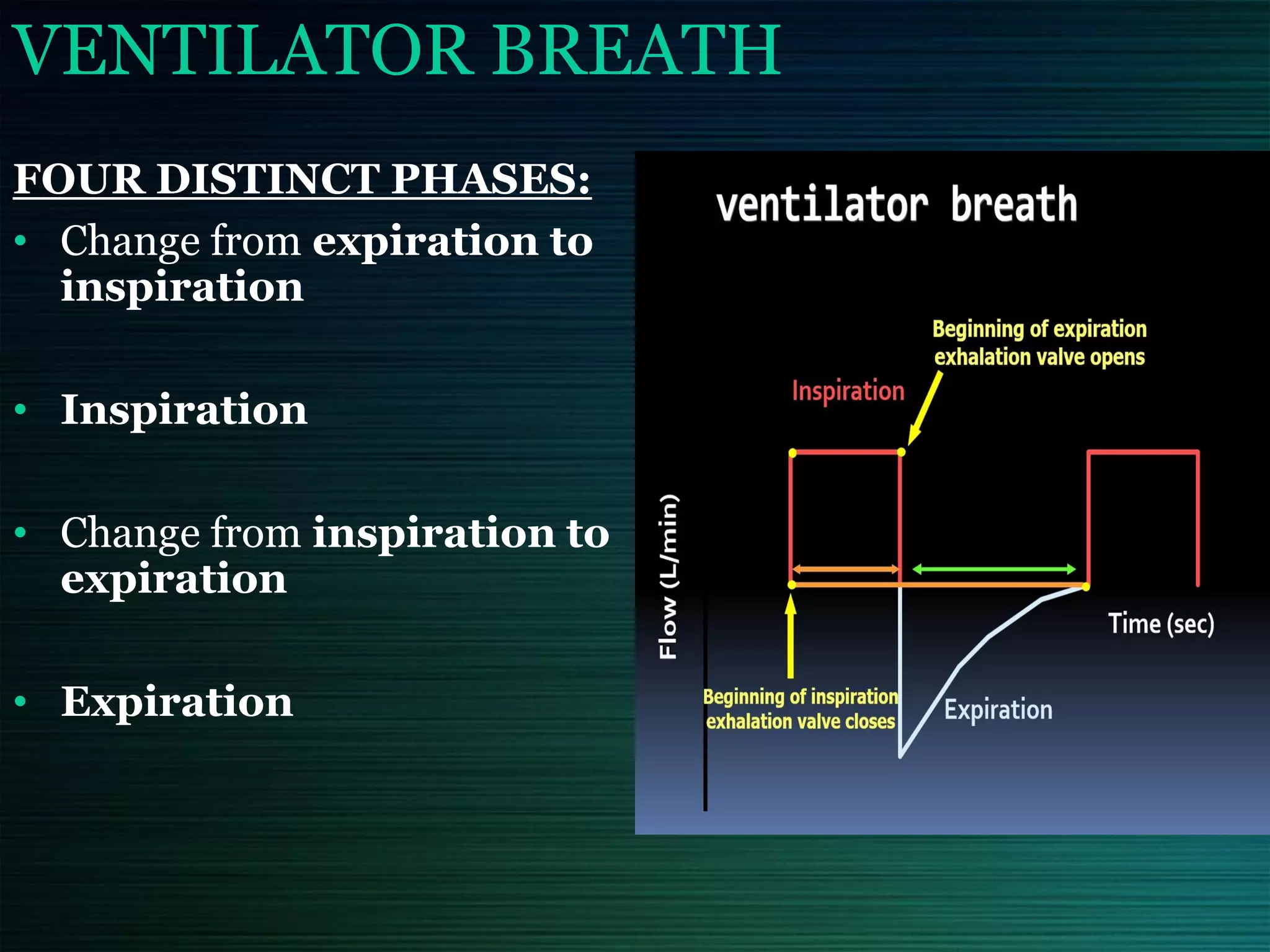
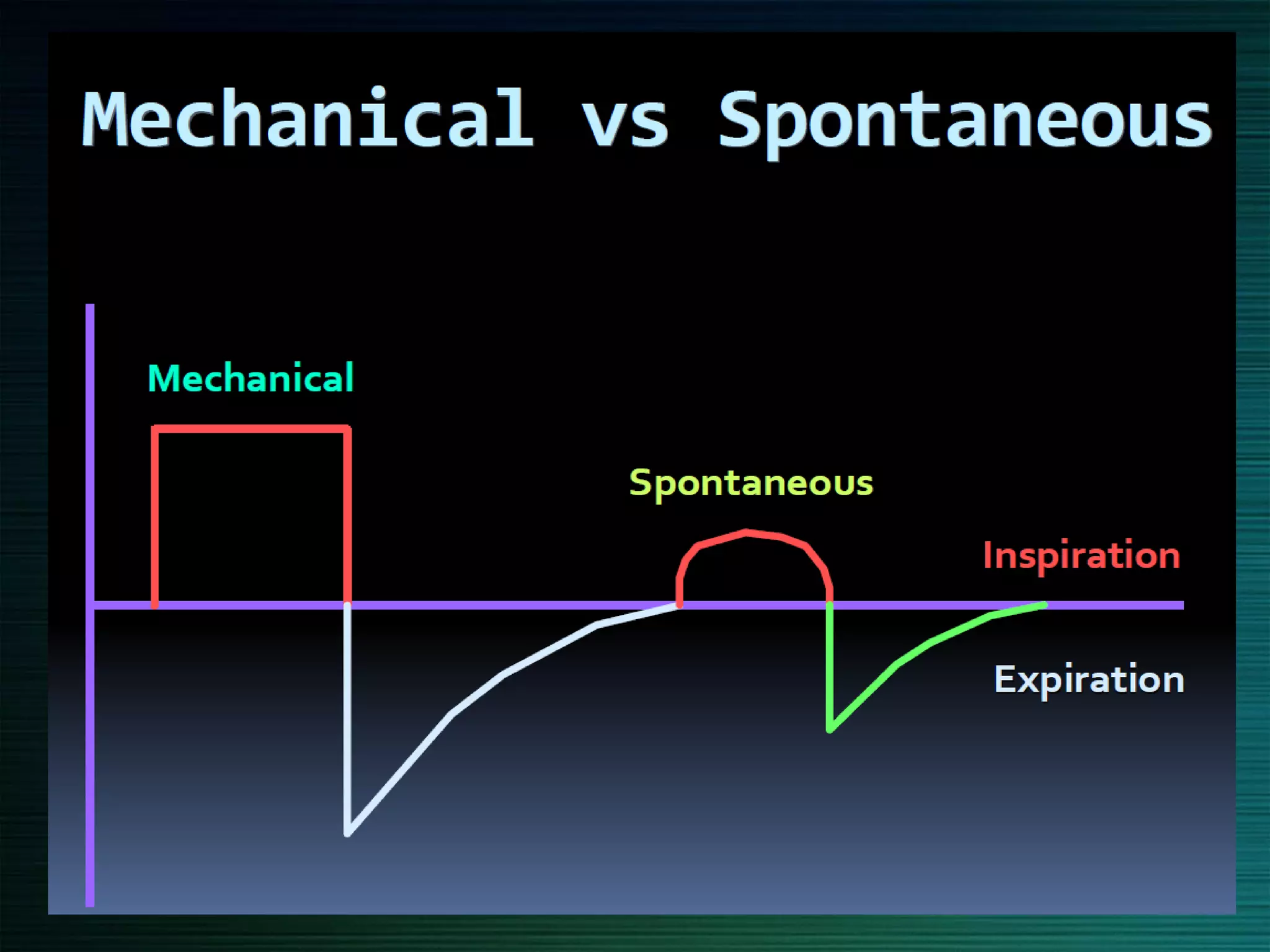
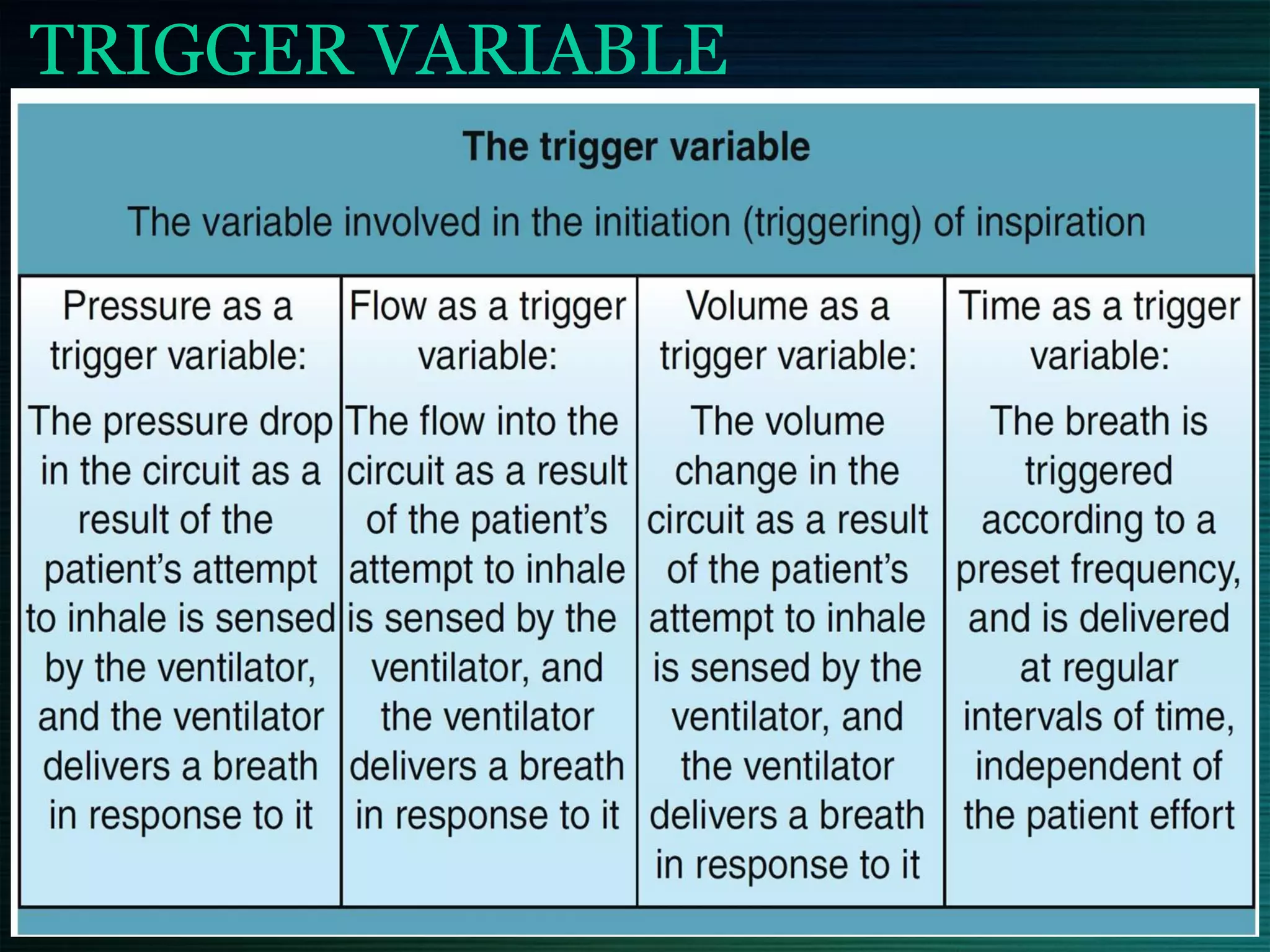
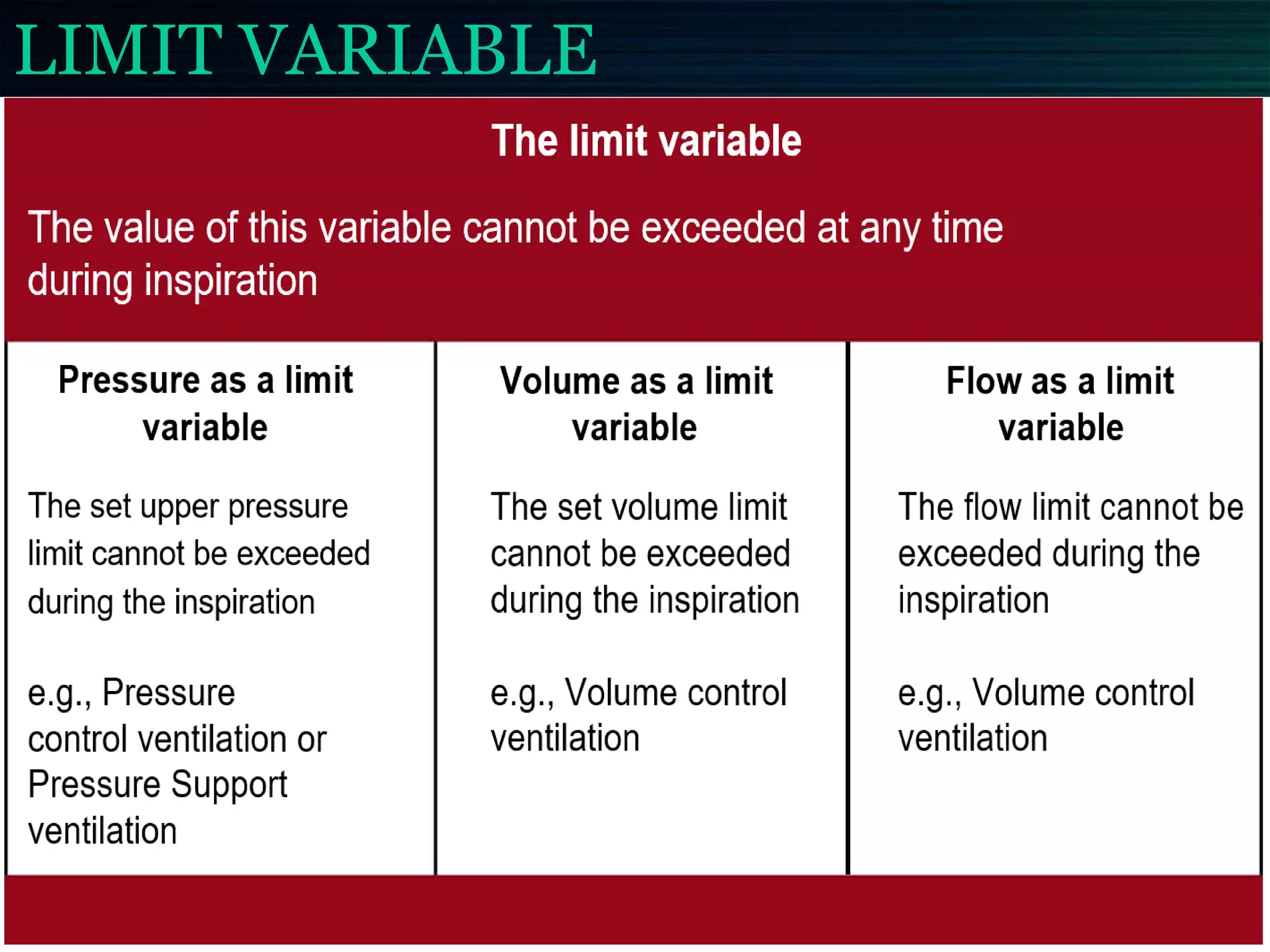
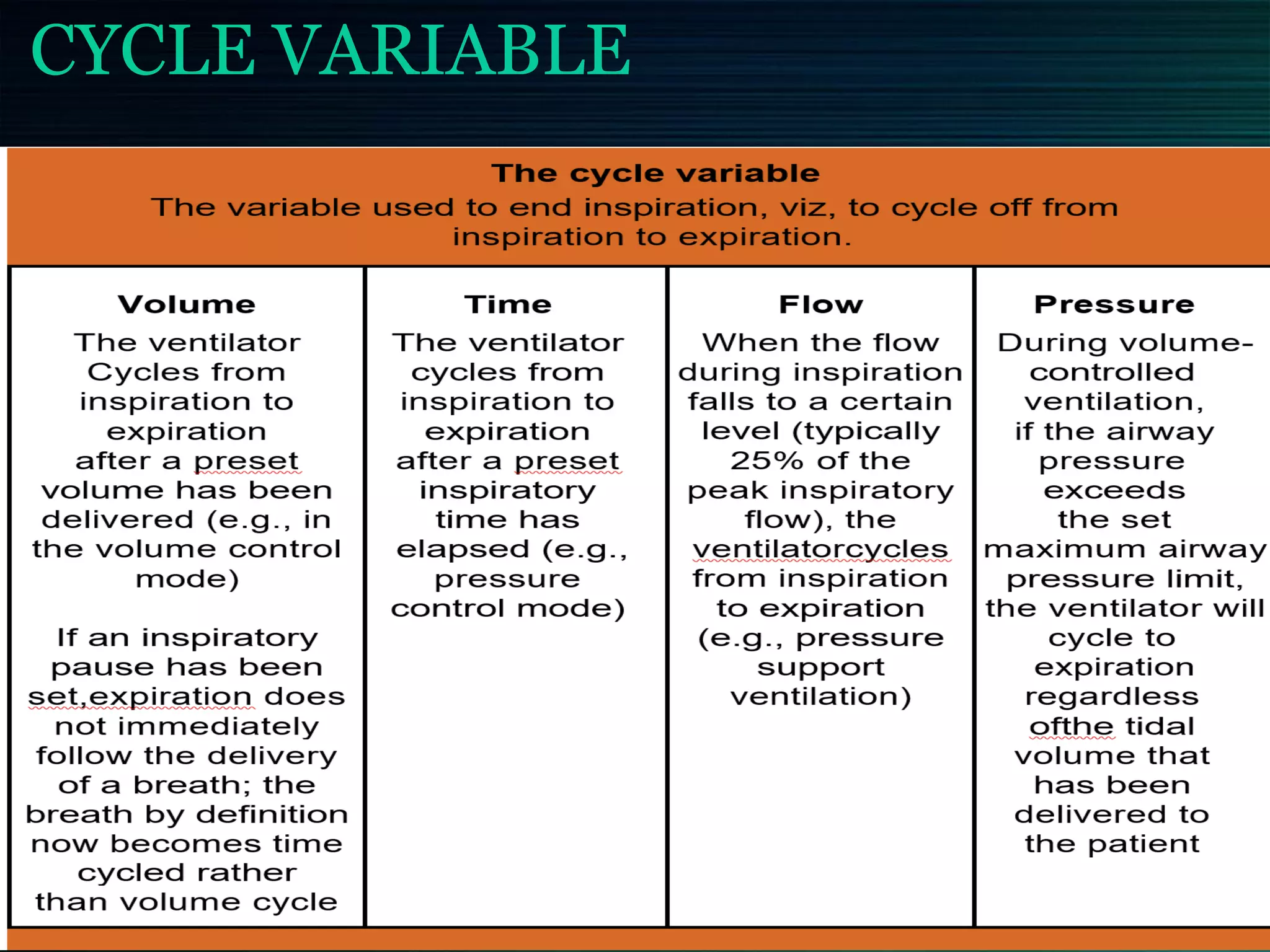
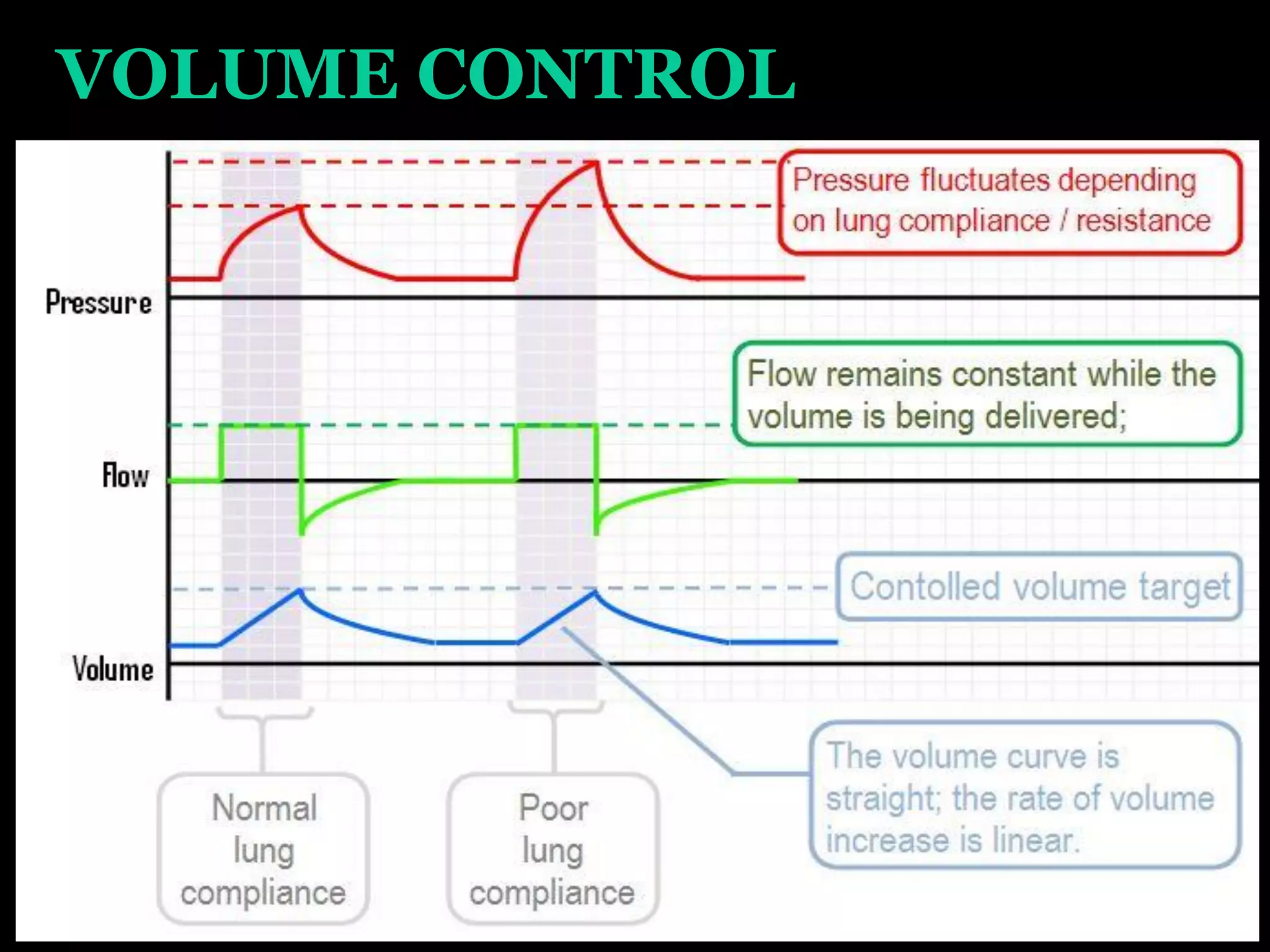
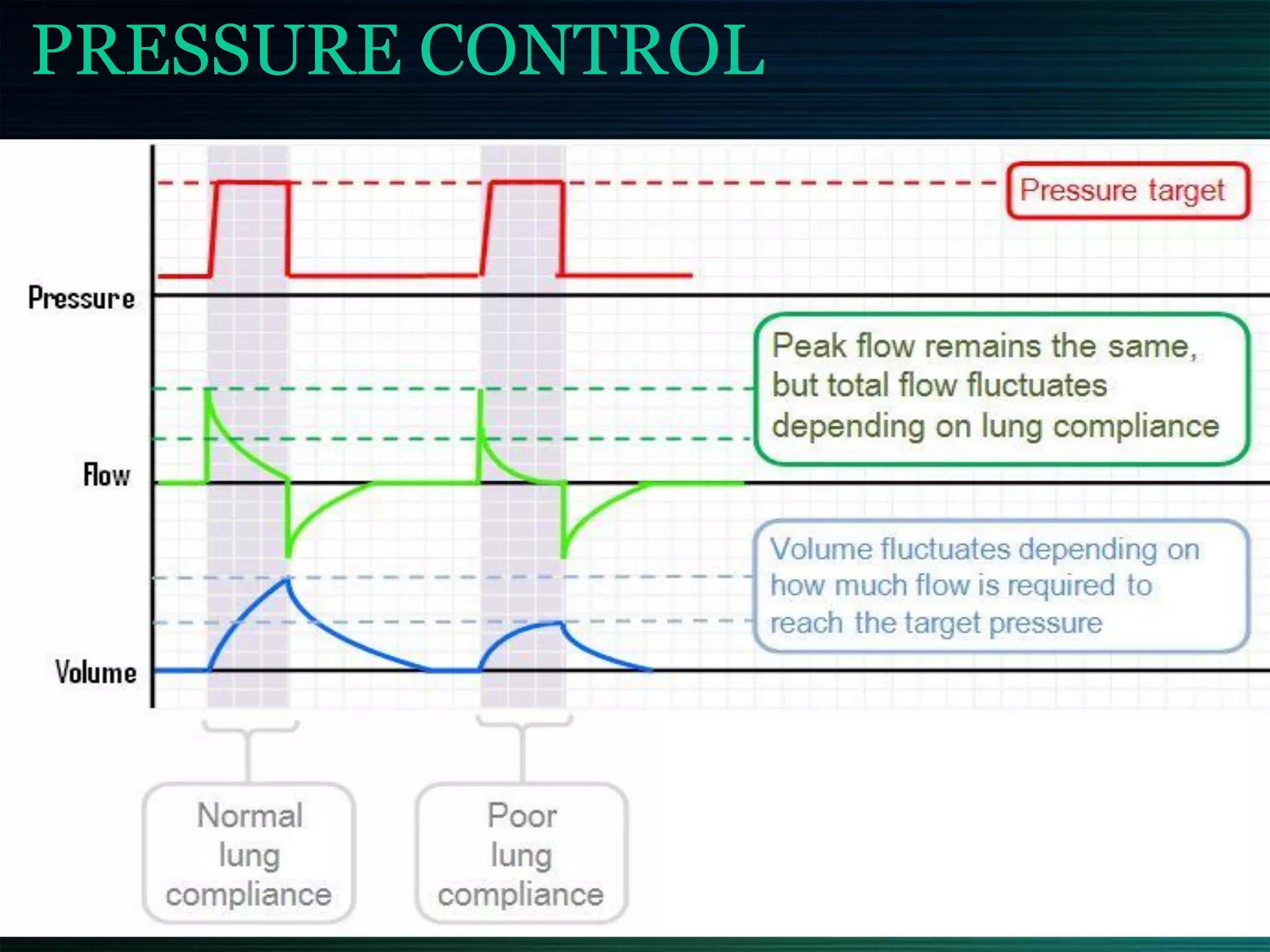
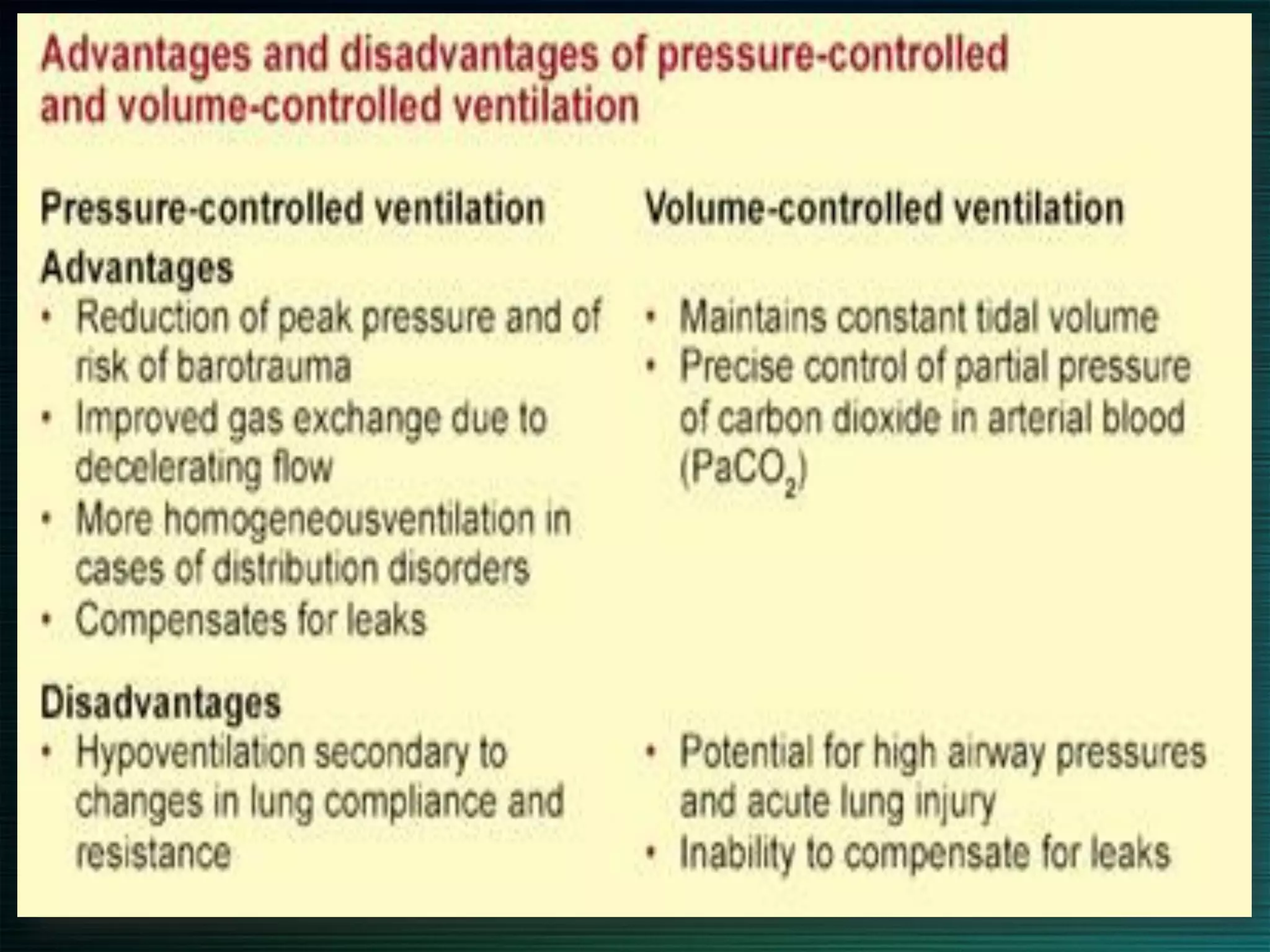
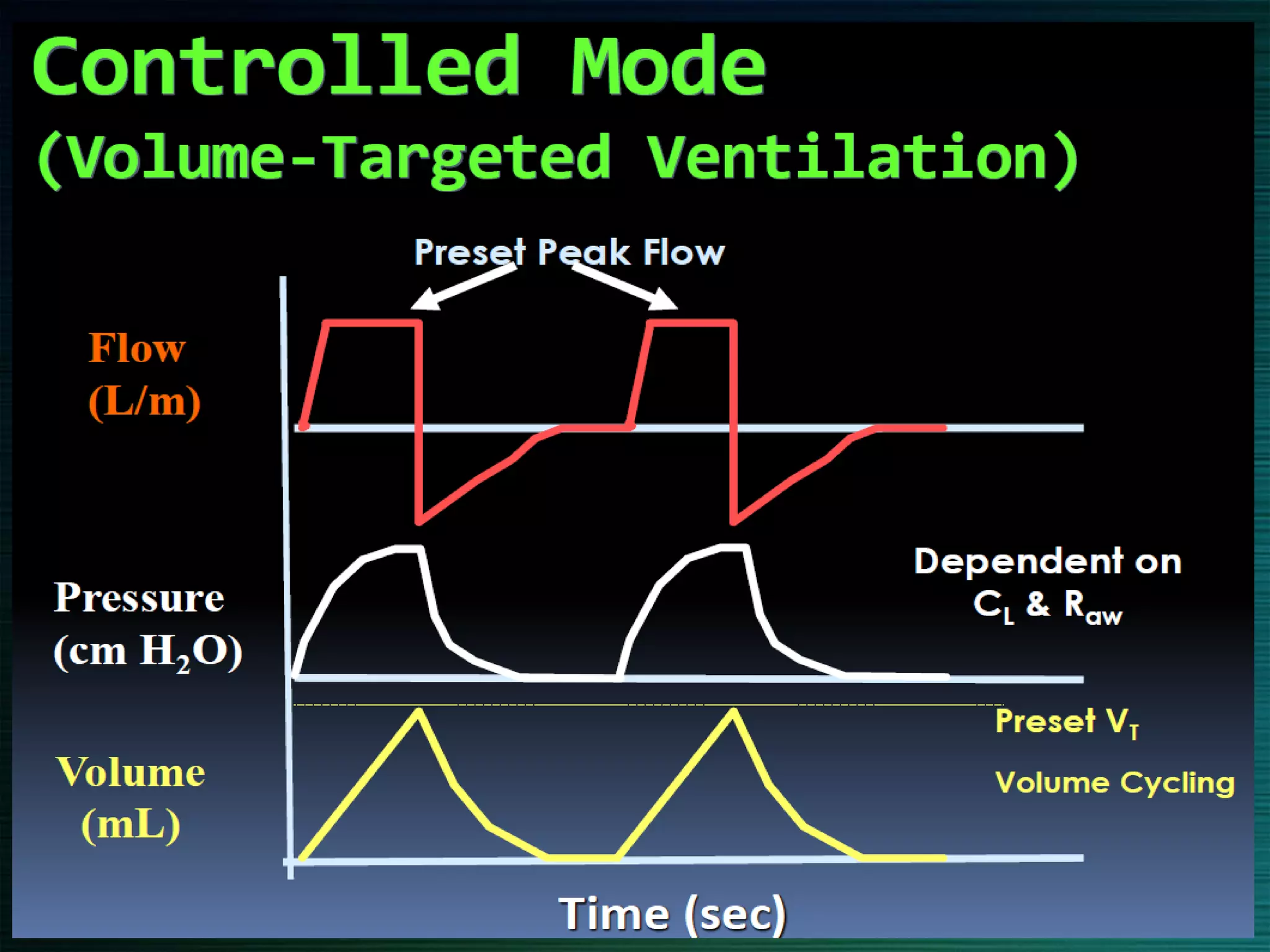
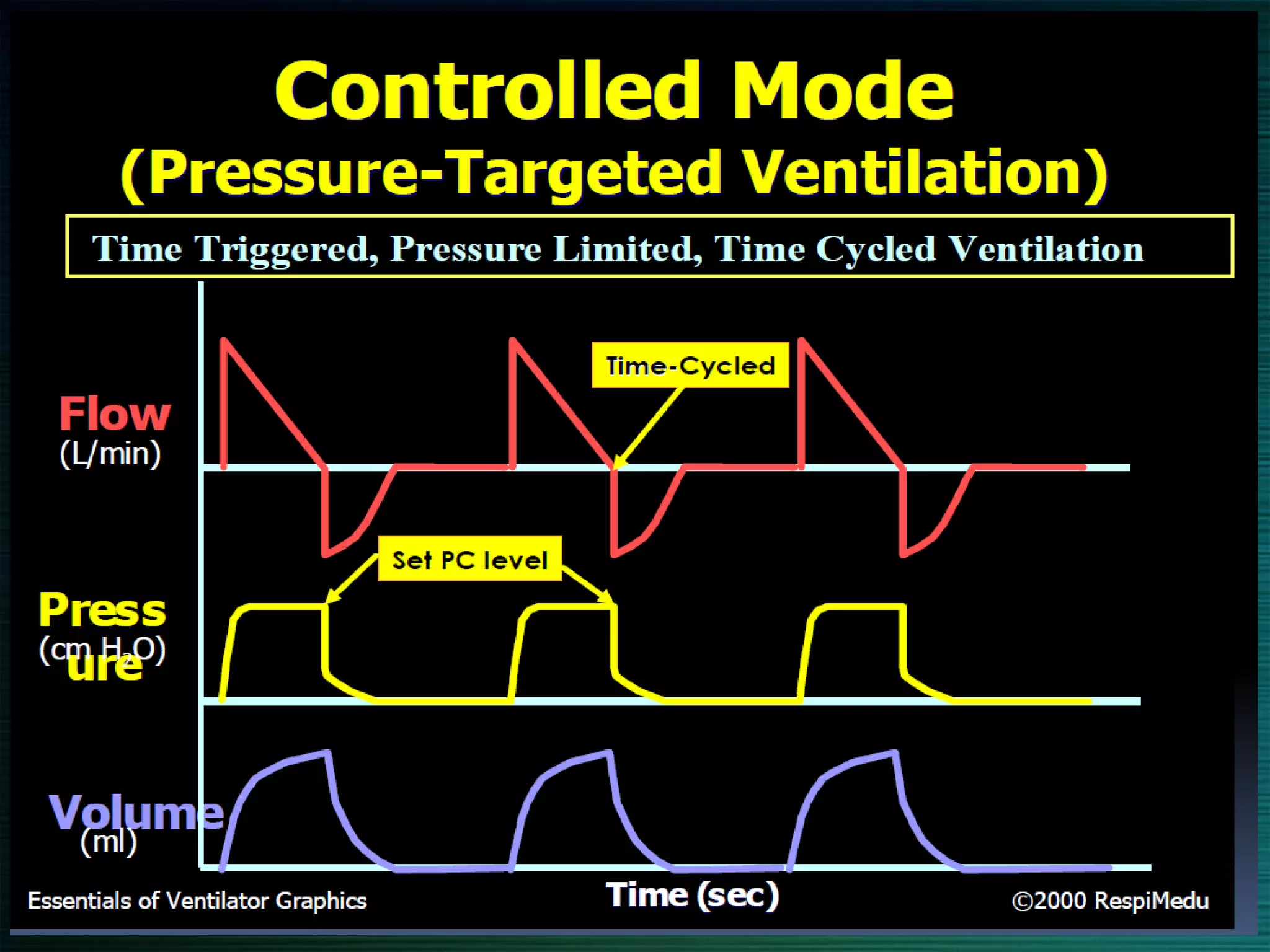
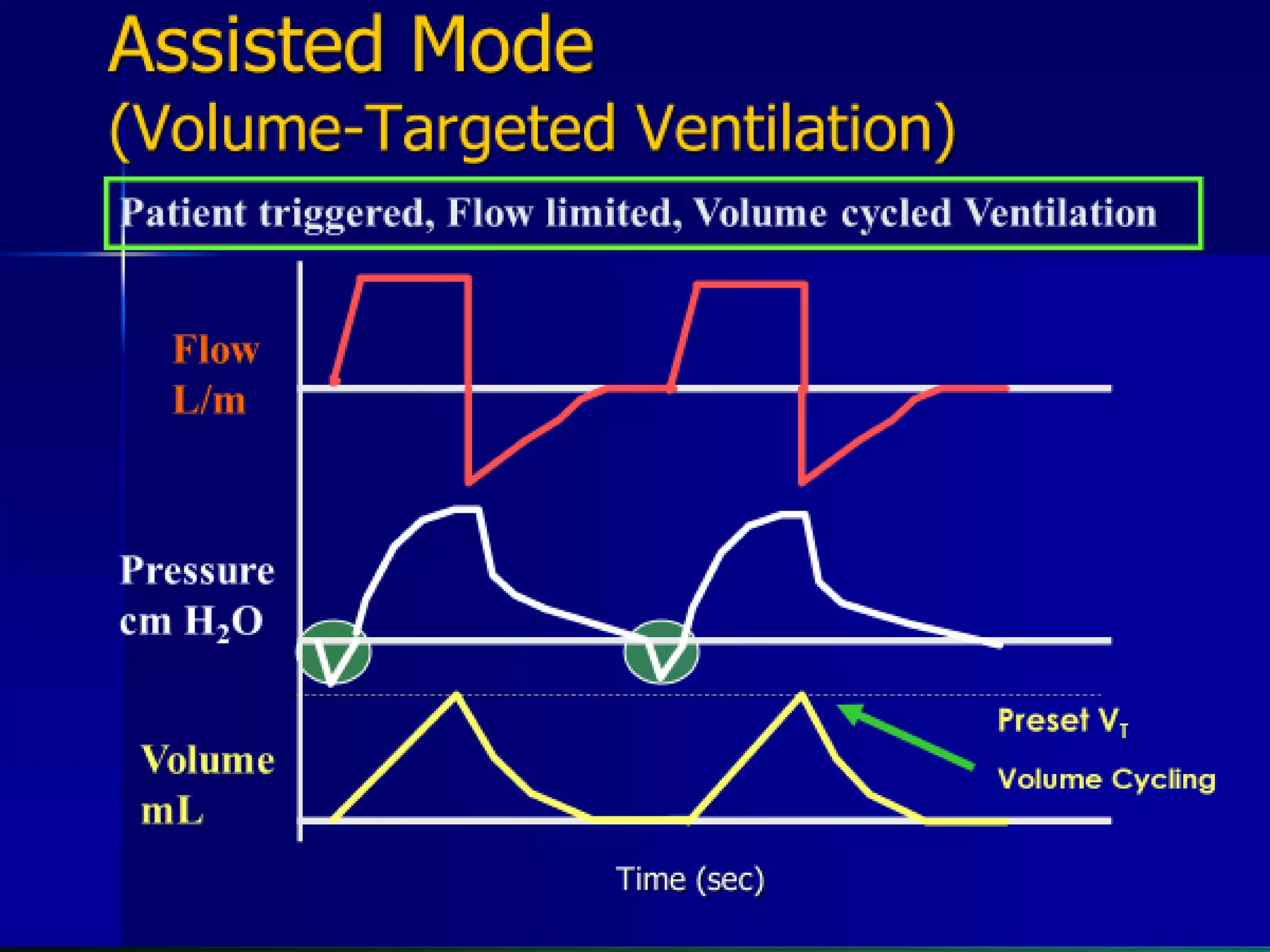
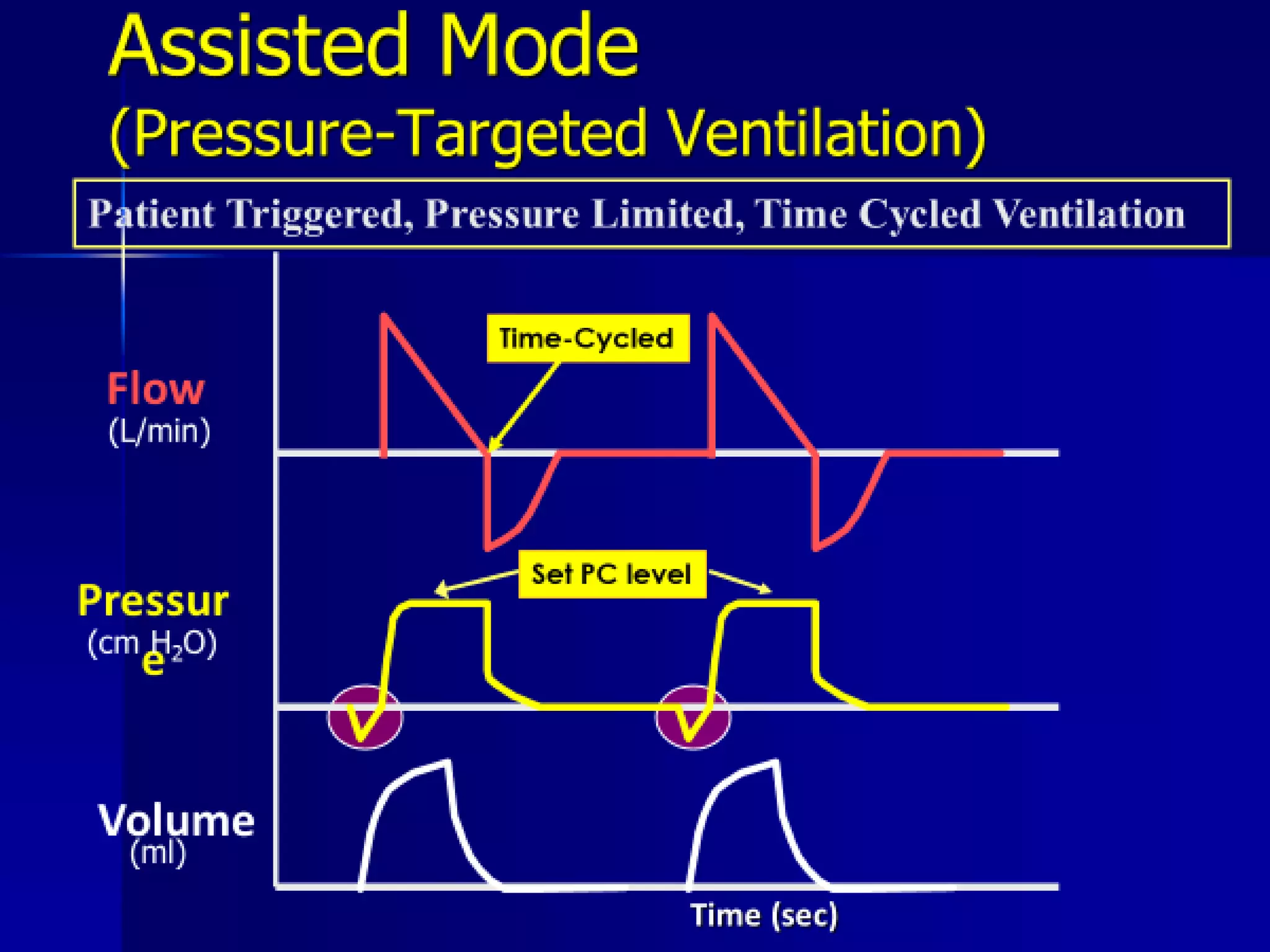

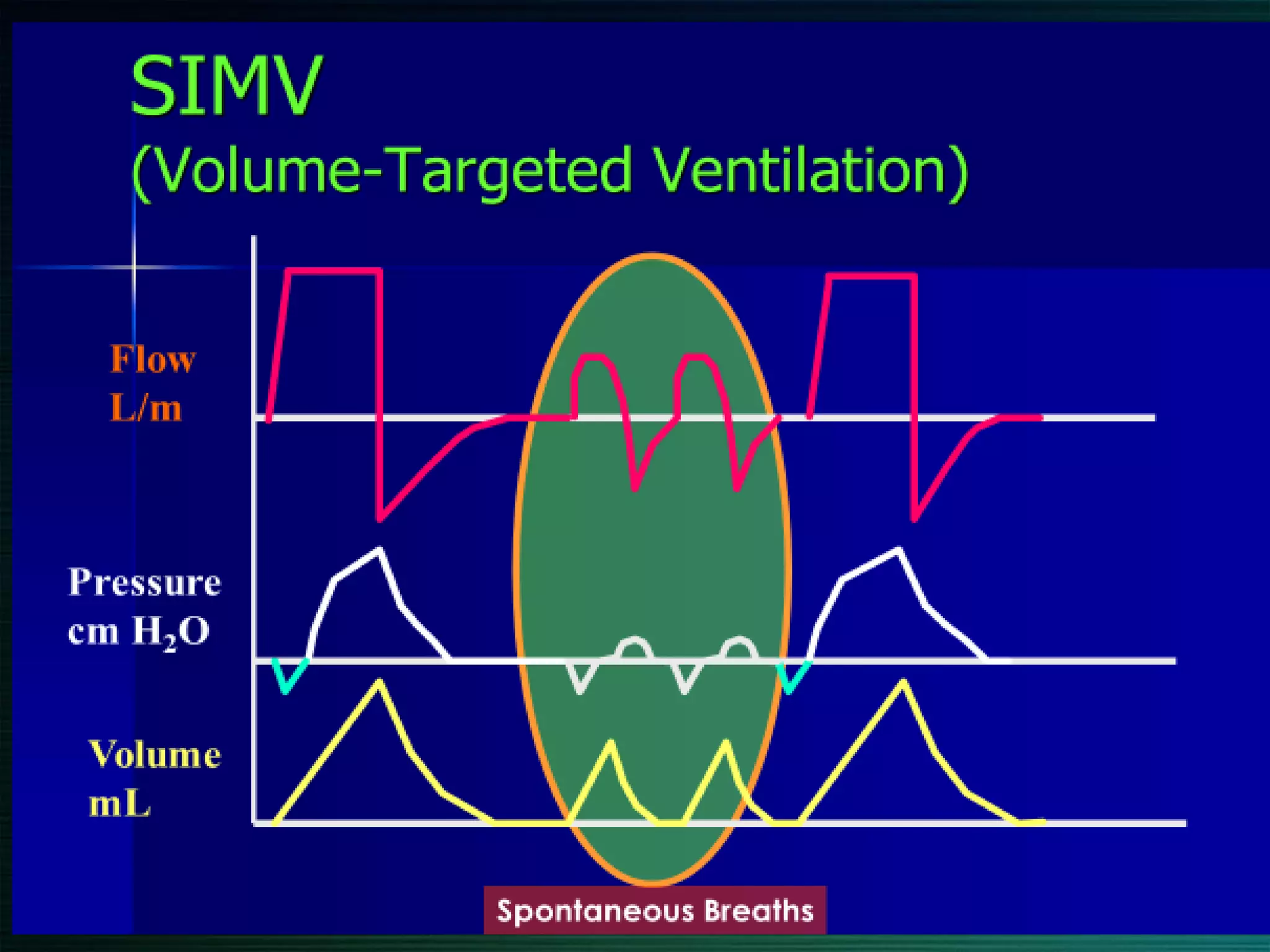
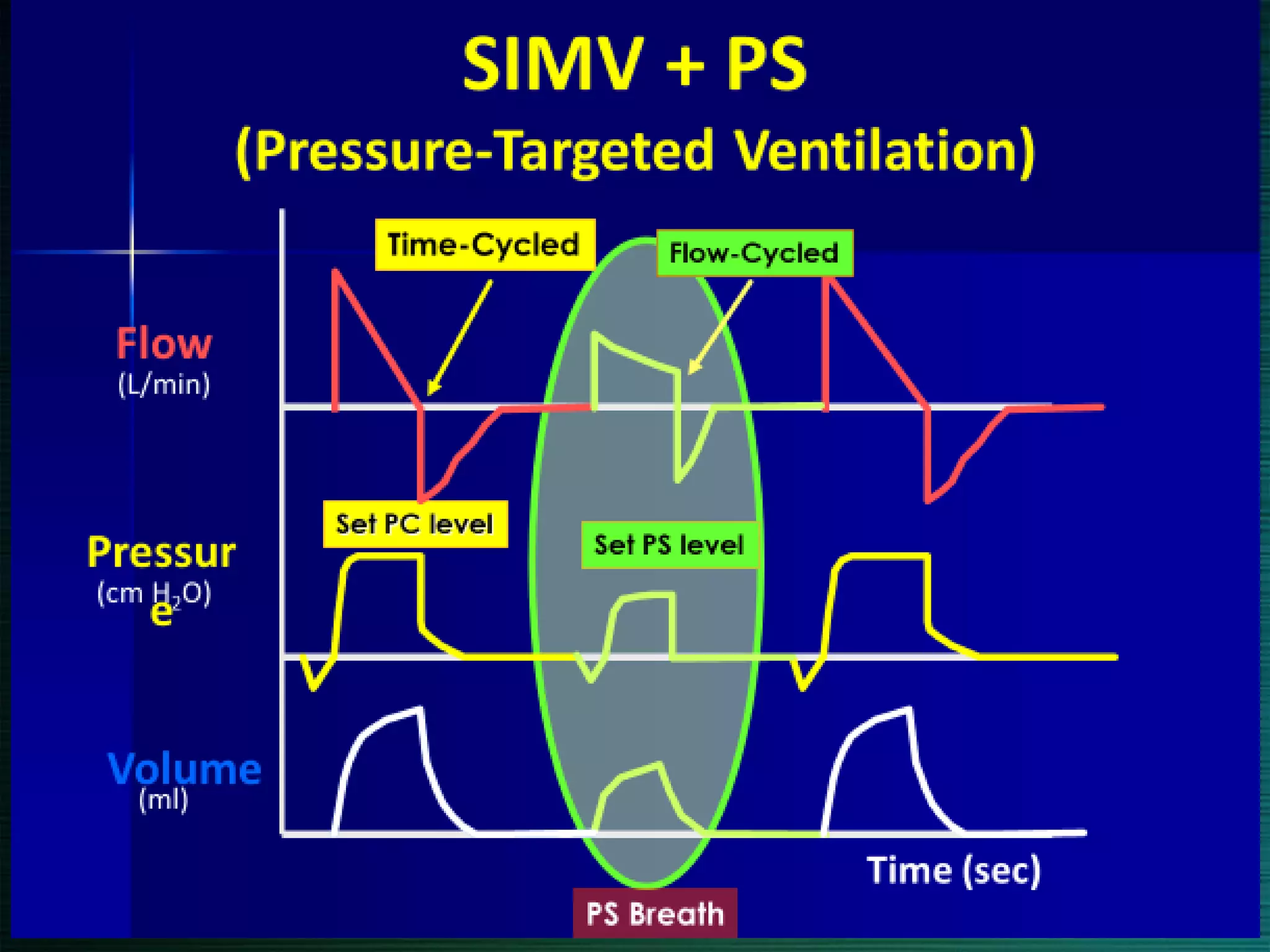






This document discusses various modes of mechanical ventilation including volume-controlled, pressure-controlled, assist-control, synchronized intermittent mandatory ventilation (SIMV), and pressure support ventilation. It defines key terms like tidal volume, respiratory rate, trigger variables, limit variables, and cycle variables. Each mode is described in terms of how breaths are triggered, the variables controlled, and whether breaths are mandatory or spontaneous.














































































