The document discusses venting. In a few short sentences, it introduces the topic of venting without providing many details. The document does not have enough context or information to generate a multi-sentence summary while maintaining accuracy.
Ventilatory Management of
ARDS(ACUTE RESPIRATORY
DISTRESS SYNDROME)
Dr. Avinash Kumar JR-2
Moderator-Dr J.N. Thakur
Dr Aditya Kejriwal
2.
Introduction
• First reportedin 1967 in adults by Ashbaugh
& coworkers
• Mortality rate of 35 to 40 %
• Death usually due to sepsis or multiorgan
faliure rather than primary respiratory
causes.
New and Improved
•Adult Respiratory Distress Syndrome
• Acute Respiratory Distress Syndrome
5.
-European Society ofIntensive Care Medicine with
endorsement from American Thoracic Society and Society
of Critical Care Medicine
-Devided three mutually exclusive severity categories:
Mild,Moderate and Severe
-Took into account: timing, chest imaging, origin of edema,
oxygenation
6.
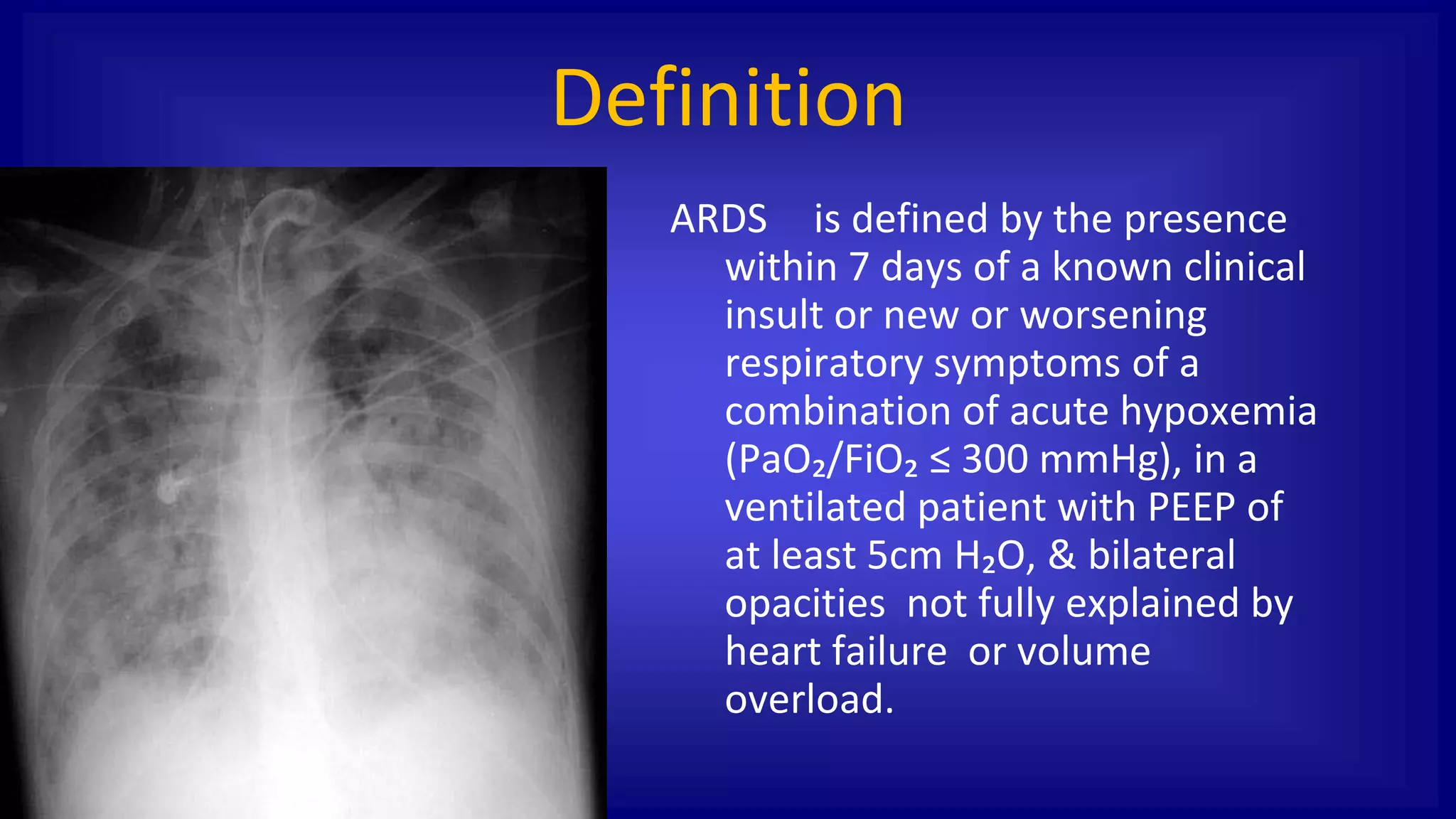
Definition
ARDS is definedby the presence
within 7 days of a known clinical
insult or new or worsening
respiratory symptoms of a
combination of acute hypoxemia
(PaO₂/FiO₂ ≤ 300 mmHg), in a
ventilated patient with PEEP of
at least 5cm H₂O, & bilateral
opacities not fully explained by
heart failure or volume
overload.
7.
Comparison of AECC& Berlin
definition of ARDS
AECC Definition Berlin Definition
Timing Acute onset Onset is within 1 week of a
Known clinical insult or new or worsening respiratory symptoms
Oxygenation ALI:PaO₂/FiO₂ ≤ 300 mmHg
ARDS:PaO₂/FiO₂ ≤ 200 mmHg
Mild: 200˂PaO₂/FiO₂ ≤ 300 mmHg with PEEP ≥ 5 cm H₂O
Moderate: 100˂PaO₂/FiO₂ ≤ 200 mmHg with PEEP ≥ 5 cm
H₂O Severe: PaO₂/FiO₂ ≤ 100 mmHg with PEEP ≥ 5 cm H₂O
Chest
Radiograph
Bilateral infiltrates Bilateral opacities not fully explained by effusions, lobar or lung
collapse or nodules
Edema PAWP ≤ 18 mmHg or no clinical
evidence of left atrial hypertension
Respiratory faliure not fully explained by cardiac faliure or
fluid overload
Risk factor Not included in definition If no risk factor for lung injury is identified then objective
assesssment like echocardiography to exclude
hydrostatic edema is needed.
8.
Clinical disorders associatedwith
development of ARDS
• Direct lung injury
– Pneumonia
– Aspiration of gastric contents
– Pulmonary contusion
– Fat emboli
– Near drowning
– Reperfusion edema (post
transplant)
– Inhalational injury
• Indirect lung injury
– Sepsis
– Severe trauma
– Cardiopulmonary bypass
– Drug overdose
– Acute pancreatitis
– Multiple blood product
transfusions
Acute Inflammation
Affects Alveolar
CapillaryMembrane
Increased
Permeability
Recruitment Of
Neutrophils
Inflammatory
Mediators
Loss Of Gas
Exchange Surface
Area
Inactivation Of
Surfactant Collapse
& Consolidation
Pulmonary Oedema
Hypoxia Pulmonary
Vasoconstriction
Profound
Hypoxaemia
Type 1 Respiratory
Failure
Patho Physiology
11.
Consequences of lunginjury include:
– Impaired gas exchange
– Decreased compliance
– Increased pulmonary arterial
pressure
– V/Q mismatch
– Increased dead space
– Impairs carbon dioxide elimination
– High minute ventilation
12.
Clinical Features ofARDS
• Rapid onset
• Severe dyspnea
• Severe tachypnea
• Arterial hypoxemia refractory to O2
therapy
• Decreased pulmonary compliance
13.
Differential Diagnosis of
ARDS
ManyDiseases Can Present Acutely With Bilateral Infiltrates and Hypoxemia
ARDS CHF Pneumonia Alveolar Hemorrhage Aspiration
T. Sisson
14.
ARDS - Principlesof Therapy
• Treat underlying cause
• Lung protective ventilation
• Promoting oxygen transport & adequate gas
exchange
• Fluid management
• Pharmacotherapy & nutrition
• Need for tracheostomy
• Avoid secondary injury & initiate mobilization
15.
Need for Mechanical
Ventilation
•Persistent hypoxemia (SpO2 ˂ 90%) on non
rebreathing facemask oxygen or NIV
• Excessive work of breathing
• Hemodynamic instability
• NIV/CPAP –limited role in immunosuppressed
• Strategy – Open up the lung & keep it open
16.
Initial ventilator settings
•Mode- VCV or PCV as starting mode
• Tidal vol.-initial 8mL/Kg PBW
• Reduce by 1mL/Kg every 2hrs until 6mL/Kg
• Inspiratory airway pressure < 30 cm H2O
• Initially high FiO2 to be titrated down with
PEEP between 5-10 cm H2O
• RR <35/min, pH goal 7.35-7.40
17.
Promoting oxygen transport
&adequate gas exchange
• Recuritment Maneuver
• Prone positioning
• High frequency
ventilation
• ECMO
• Inhaled nitric oxide
18.
ARDS Management
Mechanical Ventilation:
● Low tidal volume ventilation
● Open lung ventilation High peep
recruitment
● Inverse ratio ventilation
Unconventional approach:
● APRV
● HFV
General Measures:
● Prone positioning
● Nitric oxide
● NMBA
● Fluid Management
● ECMO
19.
Strategies of mechanicalventilation of
adults in ARDS
Low tidal volume ventilation
(lung protective ventilation)
Permissive hypercapnia
Open lung ventilation
20.
Low Tidal volumeVentilation
● Low tidal volume ventilation (LTVV) is also
referred to as lung protective ventilation.
● For patients with acute respiratory distress
syndrome (ARDS), low tidal volume ventilation (4
to 8 mL/kg PBW) is recommended
● Adjust the tidal volume to achieve an inspiratory
plateau airway pressure =30 cm H2O
21.
Low tidal volumeventilation
(LTVV)
Benefit
Evidence suggests that the early application of and
adherence to LTVV decrease mortality, as well as other
clinically important outcomes in patients with ARDS
22.
Low tidal volumeventilation (LTVV)
Benefit
● The multicenter ARMA trial randomly assigned 861
mechanically ventilated patients with ARDS to receive LTVV
(initial tidal volume of 6mL/kg PBW) or conventional mechanical
ventilation (initial tidal volume of 12 mL/kg PBW)
23.
Low tidal volumeventilation
(LTVV)
Harm
● LTVV is generally well tolerated
● It was not associated with any clinically important adverse outcomes in
the ARMA trial.
● With respect to physiologic adverse outcomes, LTVV caused
hypercapnic respiratory acidosis in some patients
● Hypercapnic respiratory acidosis was an expected and generally well
tolerated consequence of LTVV
24.
Low tidal volumeventilation (LTVV)
Harm
Two major concerns were expressed after publication of the ARMA
trial
(1) Auto-PEEP
● The higher respiratory rater in LTVV may create auto-PEEP by
decreasing the time available for complete expiration
(2) Sedation
● Work of breathing and patient-ventilator synchrony may increase when
tidal volumes are <7 mL/kg of PBW.
● While asynchrony may require increased sedation soon after the
initiation of LTVV, the need for increased sedation does not appear to
persist
Permissive Hypercapnia
● LTVVfrequently requires permissive hypercapnic ventilation (PHV), a
ventilatory strategy that accepts alveolar hypoventilation in order to
maintain a low alveolar pressure and minimize the complications of
alveolar overdistension (eg, ventilator associated lung injury)
● Hypercapnia and respiratory acidosis are a consequence of this
strategy
● Minimum accepted PH = 7.25
● The degree of hypercapnia can be minimized by using the highest
respiratory rate that does not induce auto-PEEP and shortening the
ventilator tubing to decrease dead space
27.
Open Lung ventilation(OLV)
● A strategy that combines low tidal volume ventilation (LTVV) with
a recruitment maneuver and subsequent titration of applied
PEEP to maximize alveolar recruitment
● The LTVV and set limits on plateau pressure aim to mitigate
alveolar overdistension, while the applied PEEP seeks to
minimize cyclic atelectasis.
● Together, these effects are expected to decrease the risk of
ventilator-associated lung injury.
28.
Open Lung ventilation(OLV)
● On balance, most trials do not show convincing benefit and some show
possible harm such that it is better to avoid the routine application of open
lung strategies as an initial strategy in patients with ARDS
● Any use of OLV strategies should be limited to those with severe ARDS
refractory to standard LTVV strategies; in addition, when employed
patients should be closely observed for an oxygenation response, so that
the clinician can decide whether it is appropriate to continue or abandon
the OLV trial.
29.
High PEEP
● Theroutine use of a high PEEP strategy in ARDS patients as
an initial strategy is not recommended.
● However, in patients refractory to standard methods of
mechanical ventilation, some experts use a high PEEP
strategy such as that employed in the ALVEOLI or LOVS trials
30.
High PEEP
● Itis thought that use of higher levels of PEEP benefit patients
by opening collapsed alveoli, which in turn serves to decrease
alveolar overdistension because the volume of each
subsequent tidal breath is shared by more open alveoli.
● If the alveoli remain open throughout the respiratory cycle,
cyclic atelectasis is also reduced. Alveolar overdistension and
cyclic atelectasis are the principal causes of ventilator-
associated lung injury
31.
High PEEP
● Theapplication of high PEEP does not appear to be associated
with improved mortality except perhaps in those with severe gas
exchange abnormalities
● Further study is needed to determine the optimal level of PEEP
and the ARDS population in whom a clear mortality benefit might
be expected
32.
Mode of Ventilation
●Patients with ARDS can be supported using either a volume limited or a
pressure limited mode of Ventilation
● In most patients with ARDS, a volume limited mode will produce a stable
airway pressure and a pressure limited mode will deliver stable tidal
volumes, assuming that breath to breath lung mechanics and patient effort
are stable
● Abrupt changes in the airway pressure in a patient receiving volume limited
ventilation, or in tidal volumes in a patient receiving pressure limited
ventilation, should prompt an immediate search for a cause of an acute
change in compliance
(eg, pneumothorax or an obstructed endotracheal tube)
33.
Mode Of Ventilation
●In order to adhere to a strategy of LTVV, it is probably easier to use a
volume limited approach. However, a pressure limited mode is an
acceptable alternative, as long as the resulting tidal volumes are
stable and consistent with the strategy of LTVV
● Regardless of whether volume limited or pressure limited ventilation
is chosen, fully supported modes of mechanical ventilation (eg, assist
control) are generally favored over partially supported modes (eg,
[SIMV]. This is particularly true early in the course of disease
● Ultimately, the choice of mode depends primarily on clinician comfort
and familiarity
34.
Inspiratory time adjustment
(Inverseratio ventilation)
● Refractory hypoxemia can occur even if the applied PEEP and
FiO2 are optimized. In this situation increasing the I:E ratio by
prolonging inspiratory time may improve oxygenation.
● Increasing the I:E ratio will increase the mean airway pressure
and may improve oxygenation in some patients
35.
Inspiratory time adjustment
(Inverseratio ventilation)
● There are potential costs associated with prolonging the
inspiratory time that should be considered. When the inspiratory
time is increased, there is an obligatory decrease in the expiratory
time. This can lead to air trapping, auto-PEEP, barotrauma,
hemodynamic instability, and decreased oxygen delivery.
● In addition, a prolonged inspiratory time may require significant
sedation or neuromuscular blockade. particularly if the inspiratory
time suppress the expiratory time (inverse ratio ventilation)
38.
Fluid management
• Conservativefluid management not at cost of
organ perfusion
• Both crystalloids & colloids along
with vasopressors (if required) can be
used
• Among colloid HES is Not used due risk of
renal damage
39.
Pharmacotherapy & nutrition
•Glucocoricoids
– Weigh risk & benefits for individual pts.
– To be used within 2 wks of onset
– Methlprednisolone 1mg/kg bolus followed by
1mg/kg/day infusion to be used if not on NMBA
– If no response in 5 days discontinue
– If favourable response continue for 14 days, thereafter
half dose for 7 days followed by one fourth dose for 7
days & then stop
40.
Tracheostomy
• Should beperformed once the patient is off
high Fio2 & PEEP support but still needs
continuous ventilator support due to high
Minute ventilation
41.
Weaning & mobilization
•Weaning attempts to be started once FiO2
& PEEP support decrease & minute
ventilation requirement comes down
• Early mobilization & physiotherapy to
prevent long term neuromuscular disability
42.
Benefits of Proneposition
• The dependent lung units are susceptible to collapse in
ARDS superadded by wt. Of heart ,abdominal viscera &
congested lung.
• Turning to prone alleviates the potential compressive
reduction in regional shear stress.
• Together these reduce the risk of ventilator induced
lung injury.
43.
Benefits of Proneposition
• Systemic inflammatory mediators causing organ faliure
& mortality in VILI are significantly reduced by
mechanical ventilation in prone .
• Drainage of posterior dependent lung units is improved
in prone position reducing ventilator associated
pneumonia.
• More ventilator free days in proned pts. reduces
further risk of ventilator associated pneumonia →
mortality↓
44.
Contraindication for proneposition
• Absolute
– Severe acute arrhythmia
– Pelvic fracture
– Intracranial hypertension
– Spine instability
– Recent sternotomy / heart surgery
• Relative
– Tracheostomy within first 24 hrs
– Bronchopleural fistula
– Hemoptysis/alveolar haemorrhage
– Ophthalmic surgery/increased intraocular
pressure
– Pregnancy/ intraabdominal pressure >20mmHg
45.
Complications of proneposition
• Pressure ulcers on face, chest & knee.
• ET tube obstruction, or decannulation, or extubation
( most serious/fatal event, 0-2.4%).
• Operative wound dehiscence.
• Brachial plexus injury, compression of retinal vessels.
• Diet intolerance.
• Central catheter extubation or avulsion.
• Transient desaturation & transient hypotension.
• Difficulty in instituting CPR.
46.
Summary/ Key Points
ARDSis Diagnosed by Clinical Parameters:
♦ Acute Onset in Appropriate Setting
♦ Bilateral Infiltrates
♦ Reduced Oxygenation
♦ No Evidence of CHF
Differential Diagnosis Includes:
♦ Congestive Heart Failure
♦ Alveolar Hemorrhage
♦ Pneumonia
♦ Aspiration
Pathophysiology Includes:
♦ Systemic Inflammation
♦ Injury to the Alveolar Membrane
♦ Alveolar Flooding with Plasma Fluid
♦ Inactivation of Surfactant
Respiratory Distress
↑ Resp. Rate
Hypoxemia
↓ Compliance
Bilateral
Infiltrates
47.
Summary/ Key Points
ManagementProblems:
♦ Decreased Compliance
♦ Refractory Hypoxemia
♦ High Mortality
Strategies to Manage:
♦ Decreased Compliance
♦ Refractory Hypoxemia
♦ High Mortality
Risk Factors for Mortality:
♦ Multi-organ Failure
♦ Underlying Cause of ARDS
Low Tidal Volume Ventilation
Permissive Hypercapnea
Best PEEP Curve
Prone Positioning
ECMO





















![Mode Of Ventilation
● In order to adhere to a strategy of LTVV, it is probably easier to use a
volume limited approach. However, a pressure limited mode is an
acceptable alternative, as long as the resulting tidal volumes are
stable and consistent with the strategy of LTVV
● Regardless of whether volume limited or pressure limited ventilation
is chosen, fully supported modes of mechanical ventilation (eg, assist
control) are generally favored over partially supported modes (eg,
[SIMV]. This is particularly true early in the course of disease
● Ultimately, the choice of mode depends primarily on clinician comfort
and familiarity](https://image.slidesharecdn.com/ventilotrymanagemantofards-220316110231/75/Ventilotry-managemant-of-ards-33-2048.jpg)