Downloaded 689 times




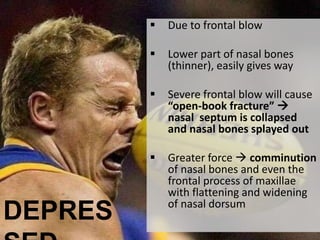



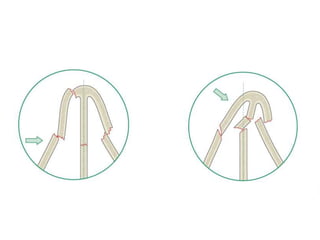
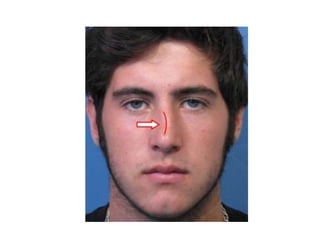






Nasal bone fractures are the most common facial trauma because the nose protrudes from the face. A frontal or lateral force can cause a nasal bone fracture depending on the magnitude. There are two main types - depressed fractures which result from a frontal blow causing the nasal bones to collapse inward, and angulated fractures from a lateral force which cause deviation of the nasal bridge. Clinical features include nasal swelling, bruising around the eyes, tenderness, deformity, and occasionally nosebleeds or nasal obstruction. Diagnosis is usually made through physical exam but x-rays can help show the fracture, though may sometimes miss it. Treatment depends on if there is displacement - non-displaced fractures may need no treatment, while displaced























































































