Overview of heart murmurs
•
14 likes•6,631 views

Summary of different heart murmurs and their features for medical finals.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (9)
Similar to Overview of heart murmurs
Similar to Overview of heart murmurs (20)
More from Christiane Riedinger
More from Christiane Riedinger (20)
Recently uploaded
Recently uploaded (20)
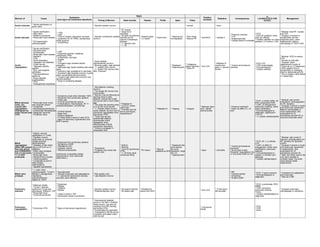
Overview of heart murmurs
- 1. Timing of Murmur Heart sounds Heaves Thrills Apex Pulse Aortic sclerosis * Senile calcification of aortic valve * Ejection systolic murmur * normal * none Aortic stenosis * Senile calcification * Bifid valve * William's syndrome * Rheumatic heart disease * DD hypertrophic cardiomyopathy * > 60y * Late! * Triad of: angina, dyspnoea, syncope * symptoms of LVF (PND, orphopnoea, frothy sputum) * Arrhythmias * Ejection (crescendo) systolic murmur * S1 normal * Quiet S2 or inaudible * S2 splits as stenosis worsens as A2 closure increasingly delayed * +/- ejection click * +/- S4 * Heaving apex * LV heave * Aortic thrill * Heaving but not displaced * Slow rising * Narrow PP * 2nd RICS * Carotid A * Pressure overload * LVH * Angina/syncope * Cardiac failure if untreated * ECG * Echo for gradient, vavle area, jet velocity * Cardiac catheter vor valve gradient, LV function, CAD * Medical: treat RF, causes and CHF * Surgical: (if severe or symptomatic as then prognosis poor): valve replacement, balloon valvuloplaty or TAVI if unfit Aortic regurgitation * Senile calcification * Bicuspid valve * Endocarditis * Rheumatic heart disease * Marfan's * EHD * Aortic dissection * Idiopathic root dilatation * Chest trauma * Takayasu arteritis, syphilis * SLE, seronegative arthritides * Pseudoxanthoma elasticum Drugs (appetite suppressants) * HTN * Osteogenesis imperfecta * Late! * Dyspnoea (pulmon. oedema), orthopnoea, PND * Arrhythmias, syncope * Angina * CCF * Corrigan's sign (marked carotid pulsation) * deMusset sign (heart nodding with every beat) * Quincke's sign (pulsations in nail beds) * Duroziez's sign (systolic murmur in groin when compressing femoral artery) * Traube's sign (pistol shot murmur over femoral arteries) * Sings of underlying disease * Early diastolic (decrescendo) murmur * Blowing quality, high pitched * +/- systolic flow murmur * +/- Austin Flint murmur (like MS), if severe! * Displaced * Hyperdynamic * Collapsing (water hammer) * Wide PP * 3rd LICS * Between R carotid and apex / L sternal border * Volume and pressure overload * ECG LVH * CXR cardiomegaly * Echocardiogram * Cardiac catheter * Medical: ACEi to reduce HTN * Monitor by echo/6m * Surgical: valve replacement if acute of >5.5cm dil or LV impairment (<55% ejection fxn) or symptomatic or enlarging heart or deteriorating ECG * Aim to replace valve before LV dysfunction Mitral stenosis (note: can coexist with regurgitation. Distinguish by pulse volume and LVH) * Rheumatic fever is the only acquired cause? * Congenital * Mucopolysaccharidoses * Endocardial fibroelastosis * Malignant carcinoid * Prosthetic valve * Symptoms onset when diameter <50% * Dyspnoea from pulmonary oedema * Chest pain * Chronic bronchitis-like picture * Complications: Haemoptysis, AF => stroke/embolisation, arrhythmias * OTHER SIGNS - Malar flush - Dilated capillaries - P mitrale (bifid p-wave) in early ECG - Signs of pulmonary hypertension and RHF if severe * Mid-diastolic rumbling murmur * The longer the murmur the more severe * Murmur may be following an opening snap in early diastole, sounds like a split 2nd sound with a much wider gap * The close the opening snap is to S2 the more severe * +/- Graham Steel murmur (early diastolic murmur due to pulmonary regurgitation from pulmonary HTN) * There may be pre- systolic/late diastolic accentuation which disappears when effectiveness of atrial contraction decreases * If there is prolapse => midsystolic click * Palpable S1 * Loud S1 unless valve rigid * If severe loud S2 due to pulmonary hypertension? * Palpable S1 * Tapping * Irregular * Between apex and L lateral sternal border - * Pressure overload? * Does not affect LV, LA only! * ECG: p mitrale (bifid), AF, RVH, progressive RAD * CXR: LA enlargement, pulmonary oedema, mitral valve calcification * Echocardiography is diagnostic: significant if <1cm^2 * +/- cardiac catheterisation * Medical: rate control (important!), anticoagulation for AF, diuretics * Surgical: If severe or acute and ventricular impairment. Balloon valvuloplasty or valve replacement. Abx prophylaxis for GI procedures (prevent IE) or recurrent rheumatic fever. Mitral regurgitation (Note: MR causes flow into atrium and FORWARDS into LV and aorta => LV NOT protected) * Elderly: annular calcification (=> CXR) * Papillary muscle dysfunction or ruptured cordae tendinae (MI/ischaemia) * Dilatation of the mitral ring in LHF/LVH or LV dilatation * Mitral valve prolapse * Endocarditis * Rheumatic fever * Marfan/Ehler's Danlos * Cardiomyopathy * Congenital as part of other cardiac malformations * Appetite supressants * Dyspnoea from pulmonary oedema * Symptoms of RHF * Palpitations (AF) * Systemic emboli * Infectice endocarditis (Ventricular contractility initially hyperdynamic, then ventricular dysfunction.) * Pansystolic * Prolapse may cause late systolic click * Soft S1 * Split S2 * Loud S2 (pulmonary HTN) * +/- S3 from rapid ventricular filling * RV heave * May be palpable as thrill * Displaced (the more severe, the more displaced / large the LV) * Hyperdynamic * Apex * Left axilla * Volume and pressure overload!? * Since there is also "forwards" regurgitation into LV and aorta, there is LVH * ECG: AF +/- p mitrale, LVH * CXR: LA AND LV enlargement, mitral valve calcification, pulmonary oedema * Echocardiography to assess LV function and aetiology * Cardiac catheterisation * Medical: rate control if required, anticoagulation for AF, diuretics for symptom control * Surgical: if severe or acute and ventricular impairment or deterioration. Abx prophylaxis for GI procedures (prevent IE) * Note: the mitral valve is the only valve suitable to consider repair, the aortic valve always needs replacement. Mitral valve prolapse * +/- ASD, PDA, cardiomyopathy, Turner's, Marfan's, osteogenesis imperfecta, pseudoxanthoma elasticum, WPW * Asymptomatic * Atypical chest pain and palppitations * +/- autonomic dysfunction (anxiety, syncope, panic attacks) * Mid-systolic click * Late diastolic murmur * MR * Cerebral emboli * Arrhytmias * Sudden death * ECG: T-wave inversion * Echocardiography is diagnostic * b-blockers for palpitations and chest pain * Rest as in MR Pulmonary stenosis * Maternal rubella * Turner's, Noonan syndrome (Turner-like phenotype), William's, TOF * Rheumatic fever * Carcinoid syndrome * Dyspnoea * Fatigue * Oedema * Ascites * Large A-wave in JVP * Dysmorphic facies if syndromic * Ejection systolic murmur * Potential ejection click * S2 quiet (if severe) * S2 widely split * Parasternal heave from RVH * 2nd LICS * To the back / left shoulder * ECG: p pulmonale, RVH, RBBB * CXR: prominent pulmonary arteries * Echo * Cardiac catheterisation is diagnostic * Surgical: pulmonary valvuloplasty or valvotomy Pulmonary regurgitation * Pulmonary HTN * Signs of pulmonary hypertension * Decrescendo diastolic murmur (1st half) = Graham Steel murmur, can also be resulting from MR causing pulmonary HTN) * Accentuated by inspiration * Compared to AR the sound is harsher and better heard with the bell * Left sternal border * ECG * CXR * Echo Murmur of Cause Symptoms (and signs not mentioned elsewhere) Signs Position (loudest) Radiation Consequences Ix ( ALWAYS ECG CXR ECHO!) Management
- 2. Pulmonary hypertension * 1* * LHF * Chronic lung disease: COPD, bronchiectasis, fibrosis, asthma, resection * Pulmonary vascular disorders: PE, vasculitis, ARDS, sickle cell, parasites * Thoracic cage malformations * MG, polio, MND * Sleep apnoea * Dysponea * Fatigue * Syncope * Cyanosis * Tachycardia * Raised JVP with prominent a and v waves * Hepatomegaly * Oedema * Pansystolic murmur from tricuspid regurgitation * Graham steel murmur from pulmonary regurgitation * Loud S2 * RV heave * FBC (2* polycythaemia?) * ABG * CXR: R heart enlargement, prominent pulmonary arteries * ECG: p pulmonale, RAD, RVH/stain * Treat cause * Treat resp. failure * Treat cardiac failure: diuretics * Venesection if polycythaemia * Heart-lung transplantation Tricuspid stenosis * Rheumatic fever * Infective endocarditis * Congenital * Rarely isolated, usually including aortic or mitral valve disease * Fatigue * Ascites * Oedema * Giant A wave of JVP, prominent Y descent * Early diastolic murmur * +/- opening snap * Left sternal edge * ECG * CXR * Echo * Medical: diuretics * Surgical: repair Tricuspic regurgitation * Dilatation of the tricuspid valve ring in RVF, e.g. due to LVF and 2* pulmonary HTN * Rheumatic fever * Endocarditis in IVDU * Carcinoid heart disease * Congenital: ASD, AV canal, Ebstein's anomaly) * Dtugs: ergot-alkaloids, fenfluramine * Giant V wave of JVP, prominent Y descent * Enlarged liver with systolic pulsation = pulsatile hepatomegaly, jaundice, ascites * Sings of RHF * Systolic brief rumbling diamond shaped or rectangular pansystolic murmur * RV heave * Marked pulsation at L lower sternal edge due to RVH) * Loudest on R costal margin * ECG * CXR * Echo * Treat underlying cause * Medical: diuretics, digoxin, ACE-i * Surgical: 10% 30d mortality! ASD * Ostium secundum defect (most common) * Ostium primum defect and associated AV valve abnormalities * Secundum defect presents late in adulthood, e.g with augmented L-R shunting in HTN * Dyspnoea * Heart failure * Pulmonary HTN * Cyanosis * Arrhythmia * Haemoptysis * Chest pain * Migraine * AF * Raised JVP * Pulmonic systolic murmur due to increased flow through the pulmonary valve * Pulmonary HTN may cause pulmonary or tricuspid regurgitation * Fixed split S2 * Eisenmenger's syndrome due to reversal of the L to R shunt by pulmonary hypertension => cyanosis * Paradoxical emboli * ECG: RBBB, LAD, long PR (primum), RAD (secundum) * CXR: small aortic knuckle, progressive atrial enlargement * Echo is diagnostic * Cardiac catheterisation: O2 sats high in R heart * In children: closure before 10y * In adults: if symptomatic * Technique: transcatheter rather than surgical VSD * Congenital * Acquired post-MI * Severe heart failure in infancy * Incidental finding * +/- signs of pulmonary hypertension * Harsh pansystolic murmur (smaller holes give louder murmurs!) * +/- L parasternal heave * Systolic thrill * L costal margin * AR * Infundibular stenosis * Eisenmenger complex * ECG: normal to LAD, LVH, RVH * CXR: cardiomegaly if severe * Echo * Cardiac catheterisation: O2 sats high in R heart * Conservative awaiting spontaneous closure * Surgical if failed medical therapy or symptomatic, IE/SCE PDA * Hypoxia in newborns * Prematurity * Iatrogenic (prostaglandins) * Dyspnoea * Tachycardia * Cyanosis (of the lower extremities) * FFT * Continuous machine-like murmur * L subclavicular thrill * Bounding pulse * Large pulse pressure * L clavicle * ECG * CXR: cardiomegaly * Echocardiogram * Conservative: waiting for closure * Medical: NSAIDS: indomethacin * Surgical: endovascular coiling or ligation Coarctation of the aorta (Most common just distal to origin of L subclavian) * Associated with bicuspic aortic valve, Turner's * Radiofemoral delay * Weak femoral pulse * HTN un upper circulation * Scapular bruit * Loud rough systolic murmur * Max over L lung anterior and posteriorly or L scapula * Heart failure * IE * CT/MRI-angiogram * CXR: rib notching * Surgical or balloon dilatation +/- stenting Pericardial friction rub * MI * Pericarditis: infectious, vascular, inflammatory, endocrine, neoplastic, traumatic, iatrogenic * Trauma * Autoimmune * Chest pain on lying flat, relieved on sitting forward * Pyrexia * 2 diastolic: when ventricles are stretched at beginning and end * 1 systolic: anywhere * High frequency murmur best heard with diaphragm * L lateral sternal border * Pericardial effusion => tamponade * Constrictive pericarditis * FBC, ESR/CRP, U&E, TFT, cardiac enzymes * ECG: saddle-shaped ST elevation +/- PR depression * CXR to rule out tamponade * Analgesia: NSAIDs * Treat cause * +/- diagnostic or therapeutic pericariocentesis Bacterial endocarditis * Note: murmurs can be mimiced by atrial myxoma * Risk factors: prosthetic valves or valvulopathy or other structal abnormality of the heart, previous rheumatic fever, IVDU, immunocompromise, DM, surgery => bacteraemia * Fever * Rigors * Night sweats * New or changing existing murmur, e.g. regurgitation * FBC, ESR/CRP * 3x blood cultures * Urine dipstick: microscopic haematuria * serology * ECG: AV block * Echo: vegetations * Empiric Abx followed by definitive * May require later surgical treatment of heart failure / valvular pathology MI * Plaque rupture + thrombosis * Embolus * Vasospasm * Vasculitis * Chest pain radiating to L arm or jaw or epigastrium * Dyspnoea * Palpitations * Anxiety * Sweating * Pallor * Vomiting * Silent: confusion/delirium, syncope, hypotension, stroke, post-op oliguria * Can present with pansystolic murmur of VSD due to ventricular rupture or pansystolic murmur of mitral regurgitation. * Can have S4 or S3 if heart failure * ECG * FBC, U&E, glucose, lipid profile, clotting * Troponin * CXR: cardiomegaly, pulmonary oedema, aortic rupture * MONABASH Morphine and metoclopramine Oxygen Nitrates Aspirin, clopidogrel Beta-blocker Ace-inhibitor Statins Heparin