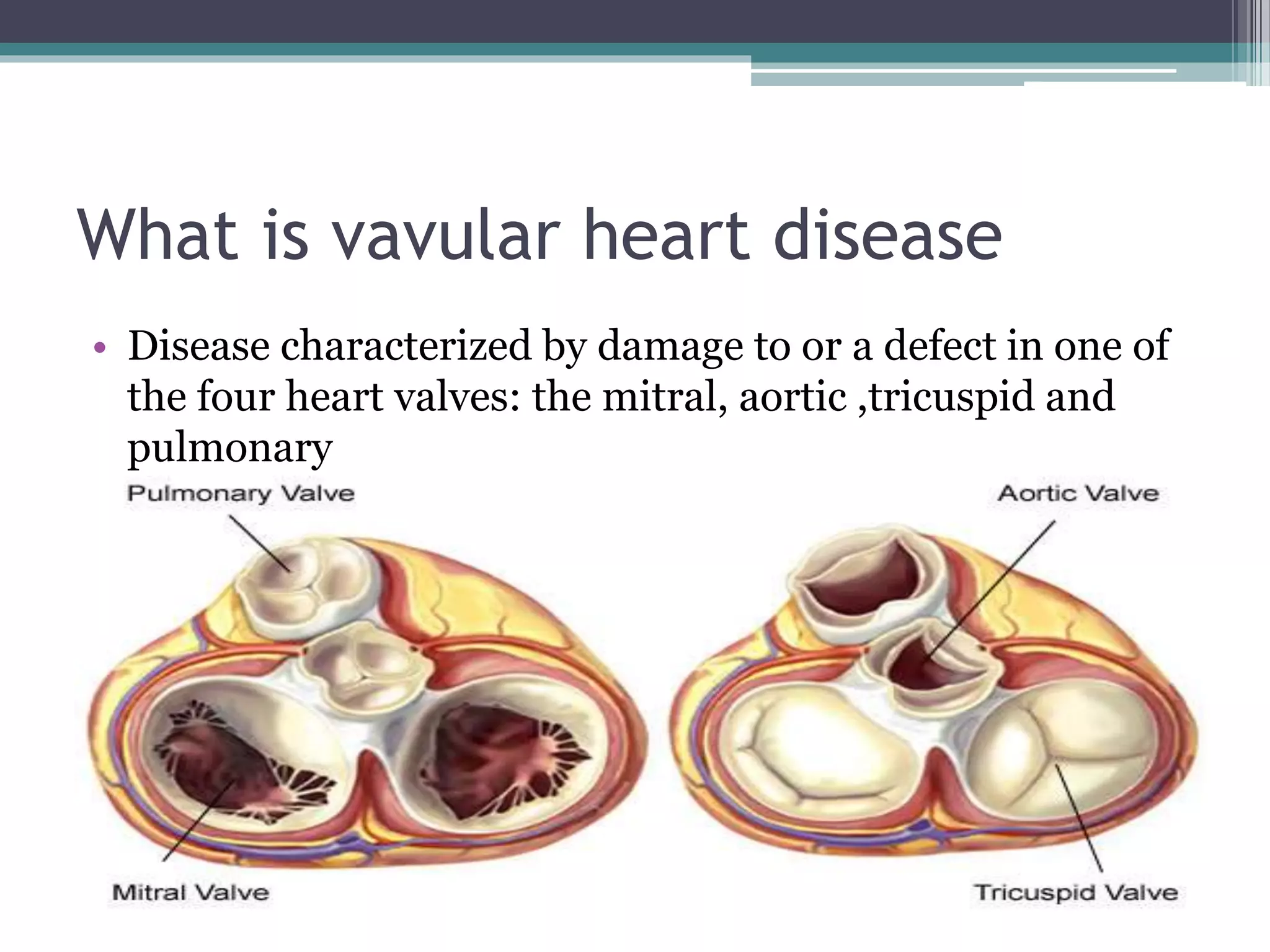
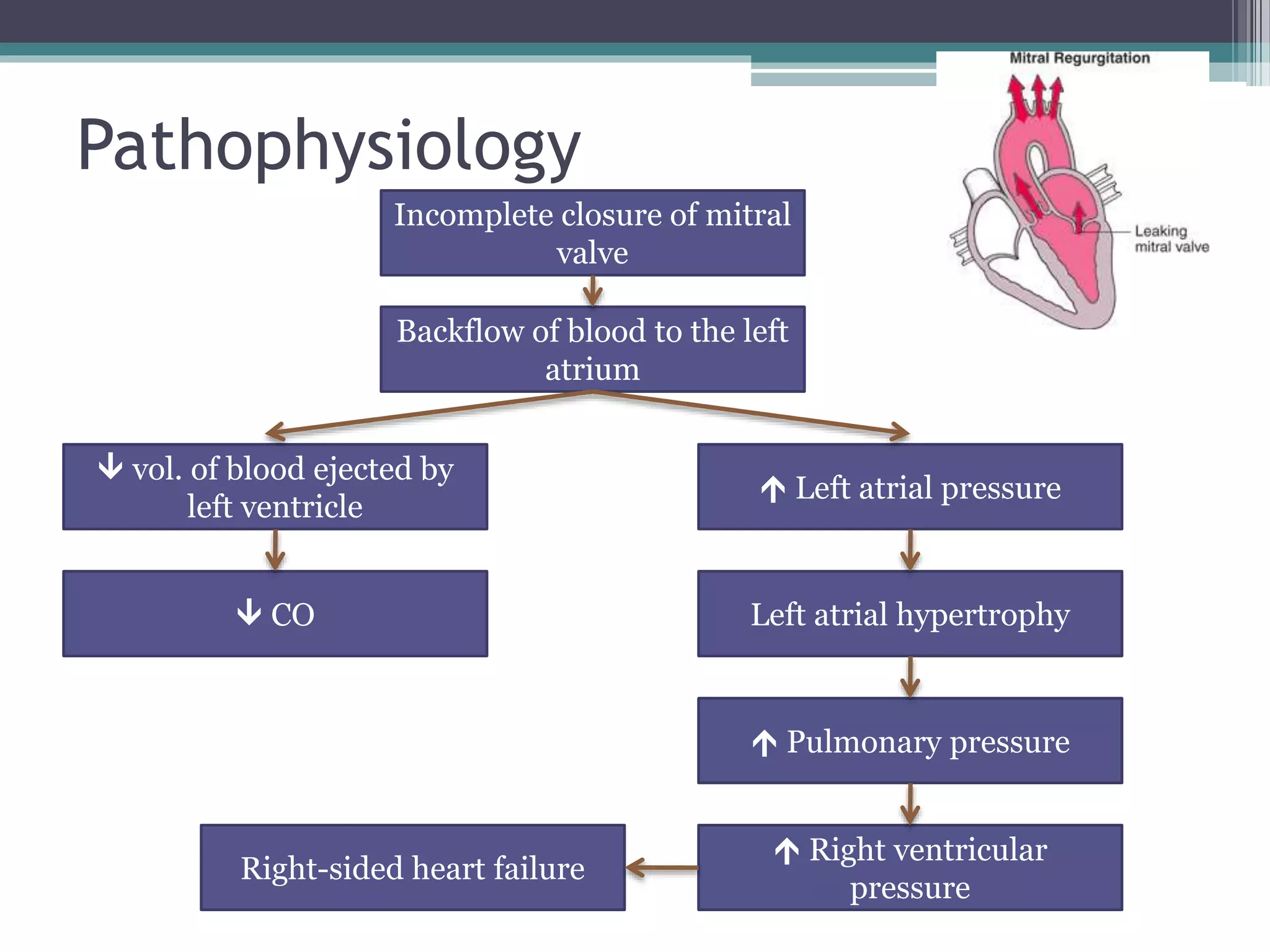
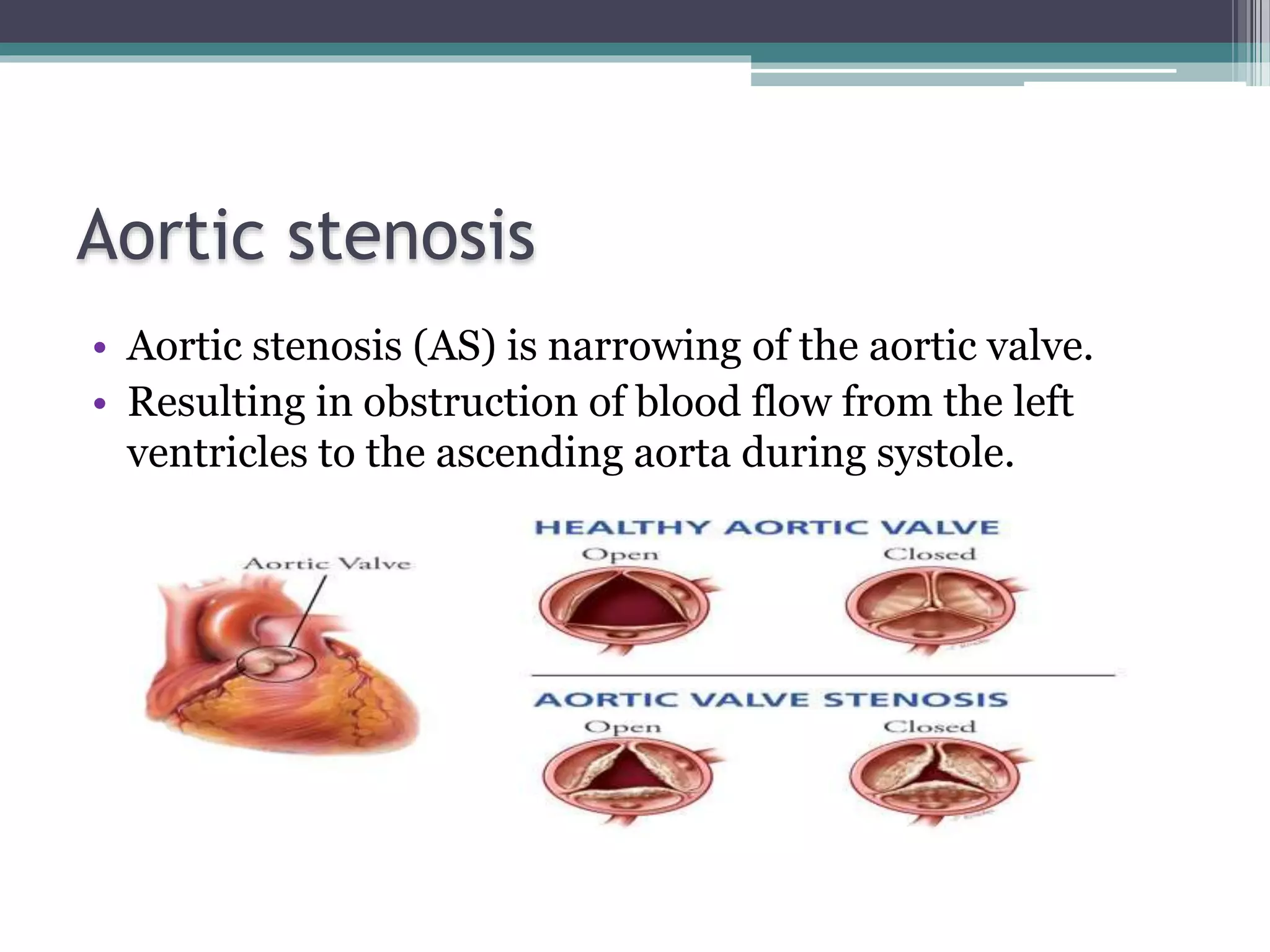
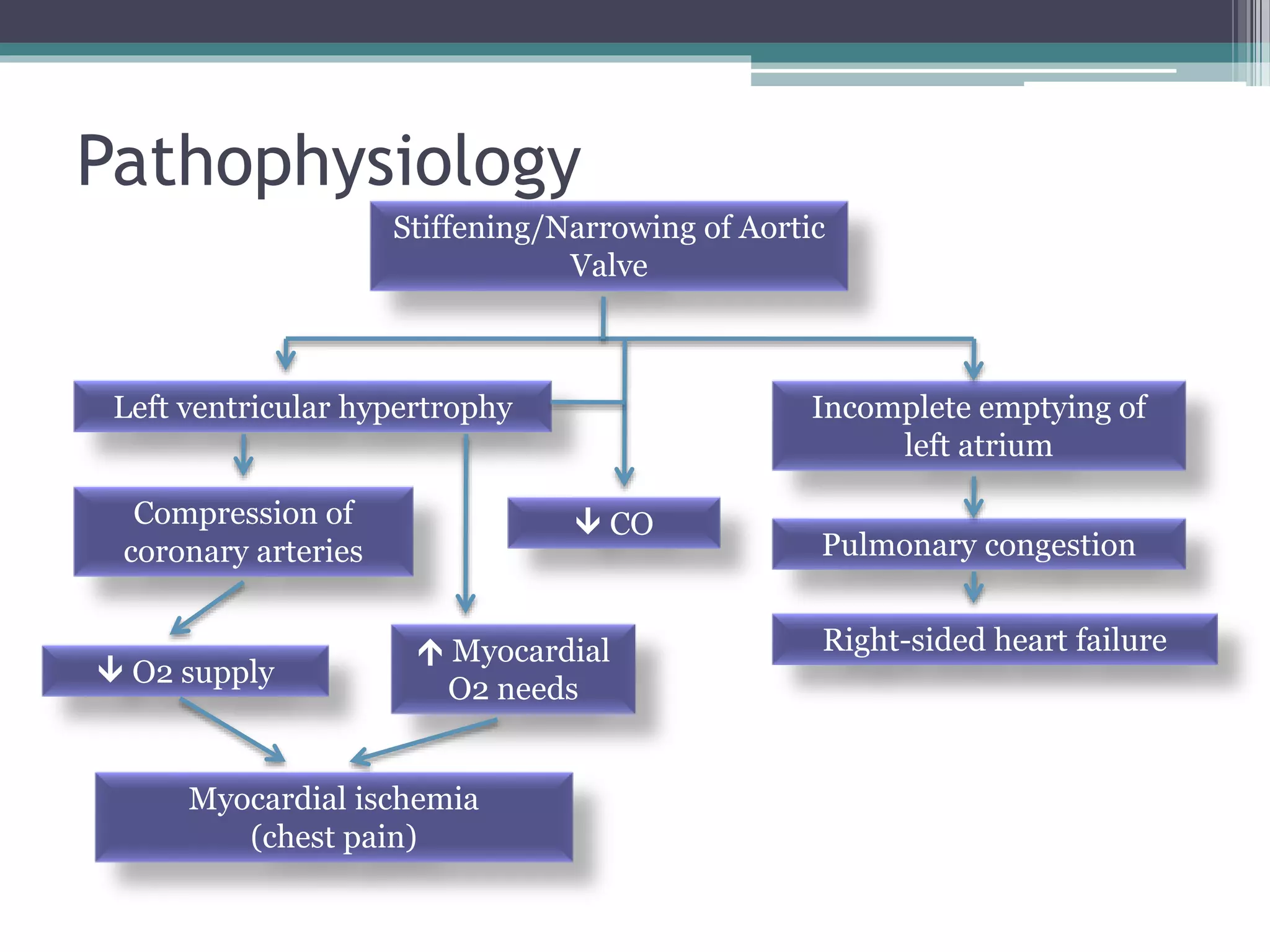
The document provides an extensive overview of valvular heart disease, detailing the types, causes, symptoms, pathophysiology, and management of conditions affecting heart valves. It covers specific ailments such as mitral stenosis, regurgitation, aortic stenosis, and others, including their clinical manifestations and diagnostic approaches. Various treatment options, including medications and surgical interventions, are also discussed for different valvular conditions.