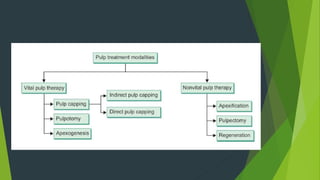
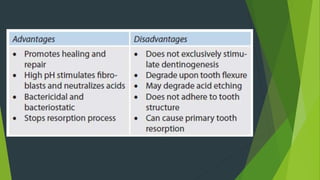
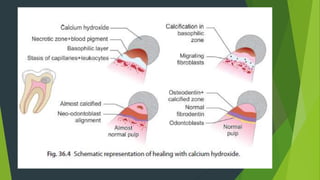
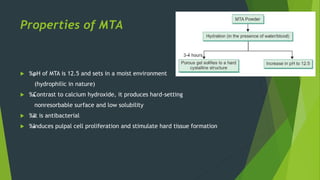
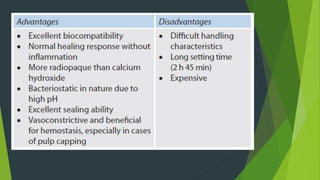
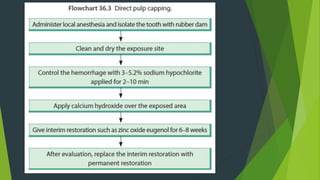
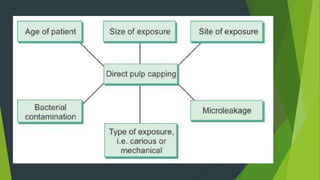
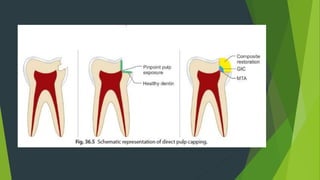
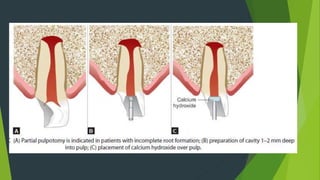
Vital pulp therapy aims to preserve pulp tissue and is especially useful for young permanent teeth due to their high healing capacity. It involves procedures like indirect pulp capping, direct pulp capping, pulpotomy, and apexification/revascularization to maintain pulp vitality and promote healing. Materials like calcium hydroxide, MTA, Biodentine, and tricalcium phosphate can be used as they are biocompatible and stimulate hard tissue formation. MTA in particular has gained popularity due to its antibacterial properties, ability to induce hard tissue formation, and creation of an apical barrier in one visit for apexification.