Downloaded 60 times

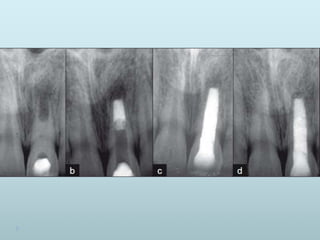
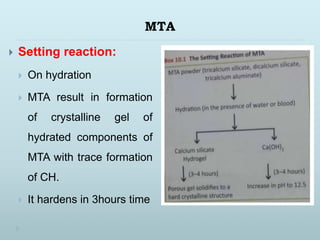

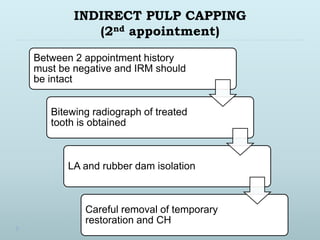
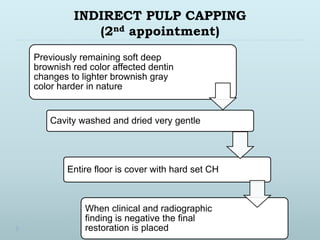
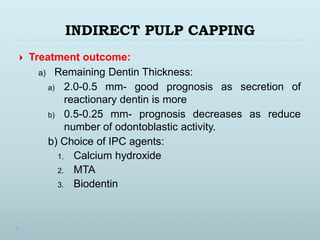

This document discusses apexification and indirect pulp capping procedures. Apexification is used to induce calcification at the open apex of an immature tooth to allow for root canal treatment. Materials used include calcium hydroxide, tricalcium phosphate, and MTA. Calcium hydroxide is placed in the canal and replaced every 3 months until radiographic evidence of apical barrier formation. MTA can also be used by placing it at the apex. Indirect pulp capping covers the deepest carious dentin with a biocompatible material like calcium hydroxide to prevent pulpal exposure while removing infected dentin, allowing for pulp preservation.





















































































