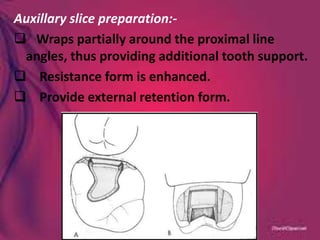
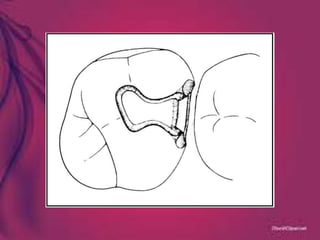
This document provides an overview of cast metal restorations, specifically class II inlay cavity preparation. It discusses the introduction of inlays in dentistry, materials used for cast metal restorations, definitions, indications and contraindications. It also covers principles of cavity preparation, types of bevels and flares, tooth preparation for class II inlay cavities, and modifications that can be made.






































![Differences-Between-Cast-Restoration-and-Amalgam[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/411598117-differences-between-cast-restoration-and-amalgam1-240425113051-8a78e12c-thumbnail.jpg?width=640&height=640&fit=bounds)





![CAST_RESTORATIONS..................................[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/castrestorations1-251004081334-a7315aa9-thumbnail.jpg?width=640&height=640&fit=bounds)


































