Downloaded 34 times







![Diagnosis &Investigation
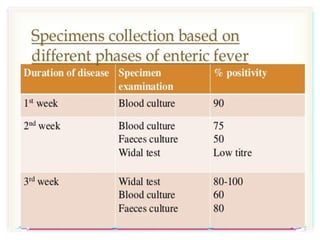
• Blood culture
• Specific serologic test
Identify Salmonella antibodies / antigens
[ Fluorescent antibody study to look for
substances that are specific to Typhoid
bacteria ]
Widal Test and ELISA
• Urine and Stool Culture (2nd & 3rd week)
• Marrow Culture *
- 90% sensitive unless until after 5
days commencement of antibiotic
- obtained from CSF, peritoneal
fluid, mesenteric LNs, resected intestine,
gallbladder, pharynx, tonsils, abscess,
bone
• Punch-biopsy samples of rose spots Culture
- 63% sensitive](https://image.slidesharecdn.com/typhoid-210203183943/85/Typhoid-17-320.jpg)



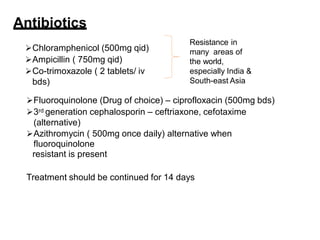


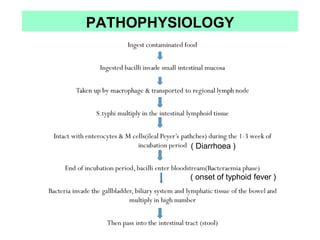
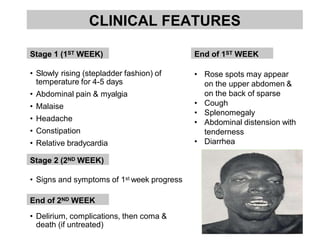
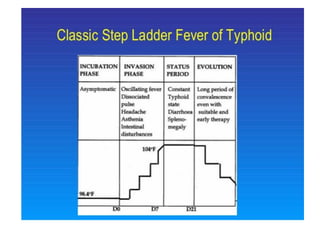
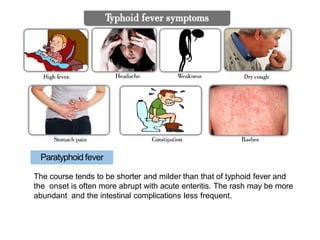
Typhoid fever is caused by infection from the Salmonella typhi bacteria. It is spread through contaminated food or water. Symptoms include a sustained fever, abdominal pain, and headache. Without treatment, some patients may develop severe complications like intestinal bleeding or perforation. Diagnosis involves blood or stool cultures. Treatment is with antibiotics like fluoroquinolones for 2 weeks. A small percentage of patients become chronic carriers even after treatment.














































































