
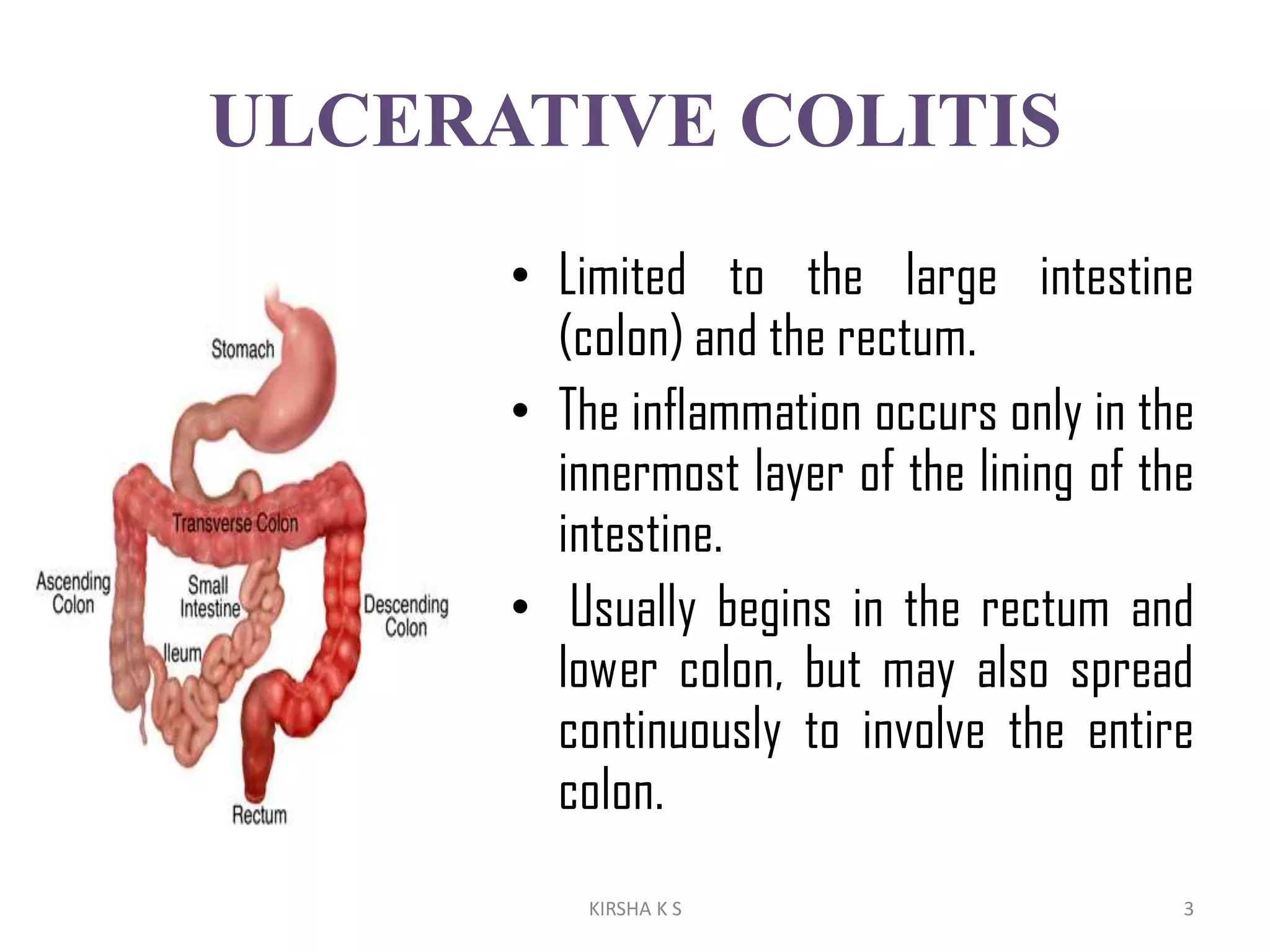
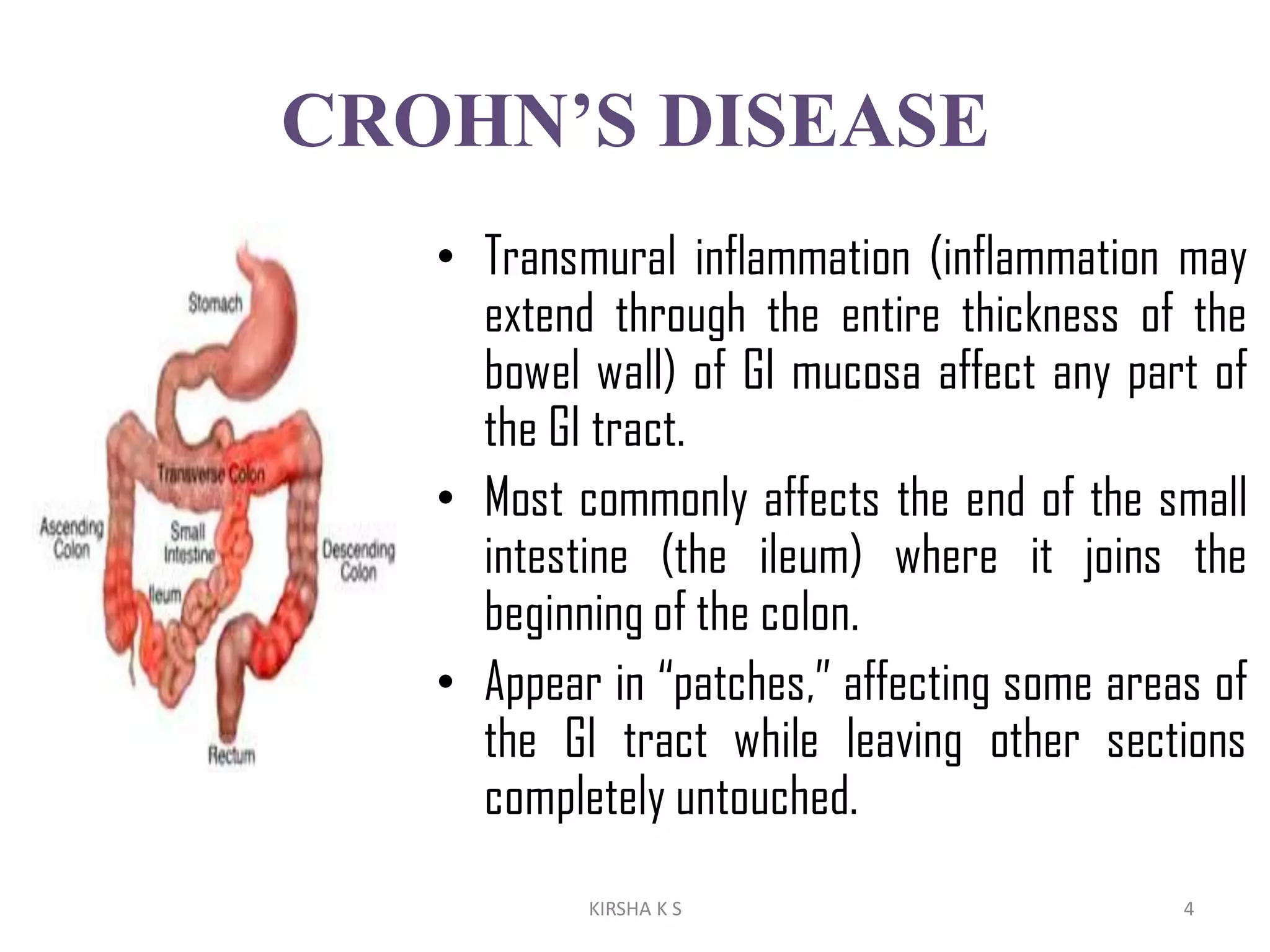



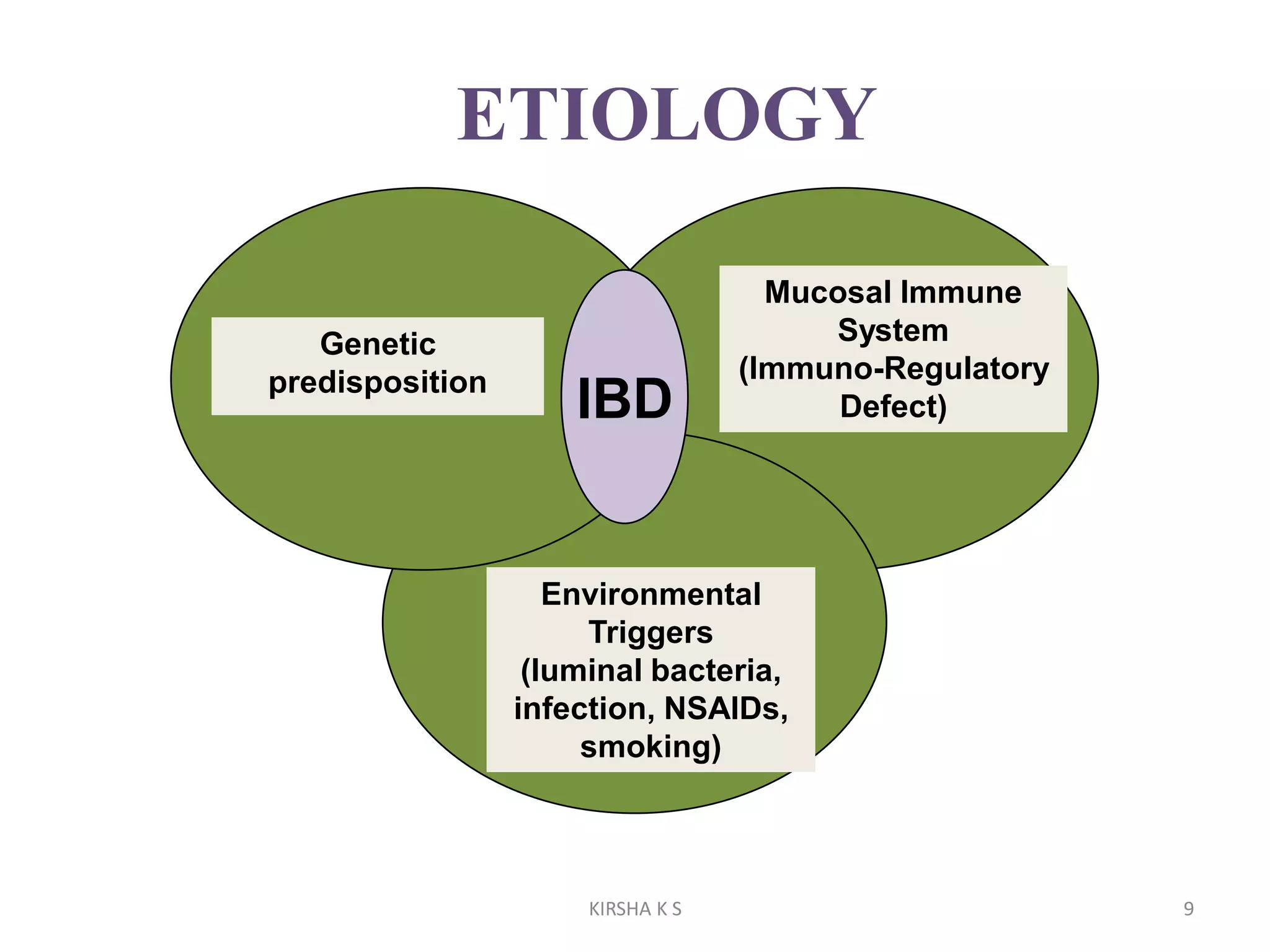




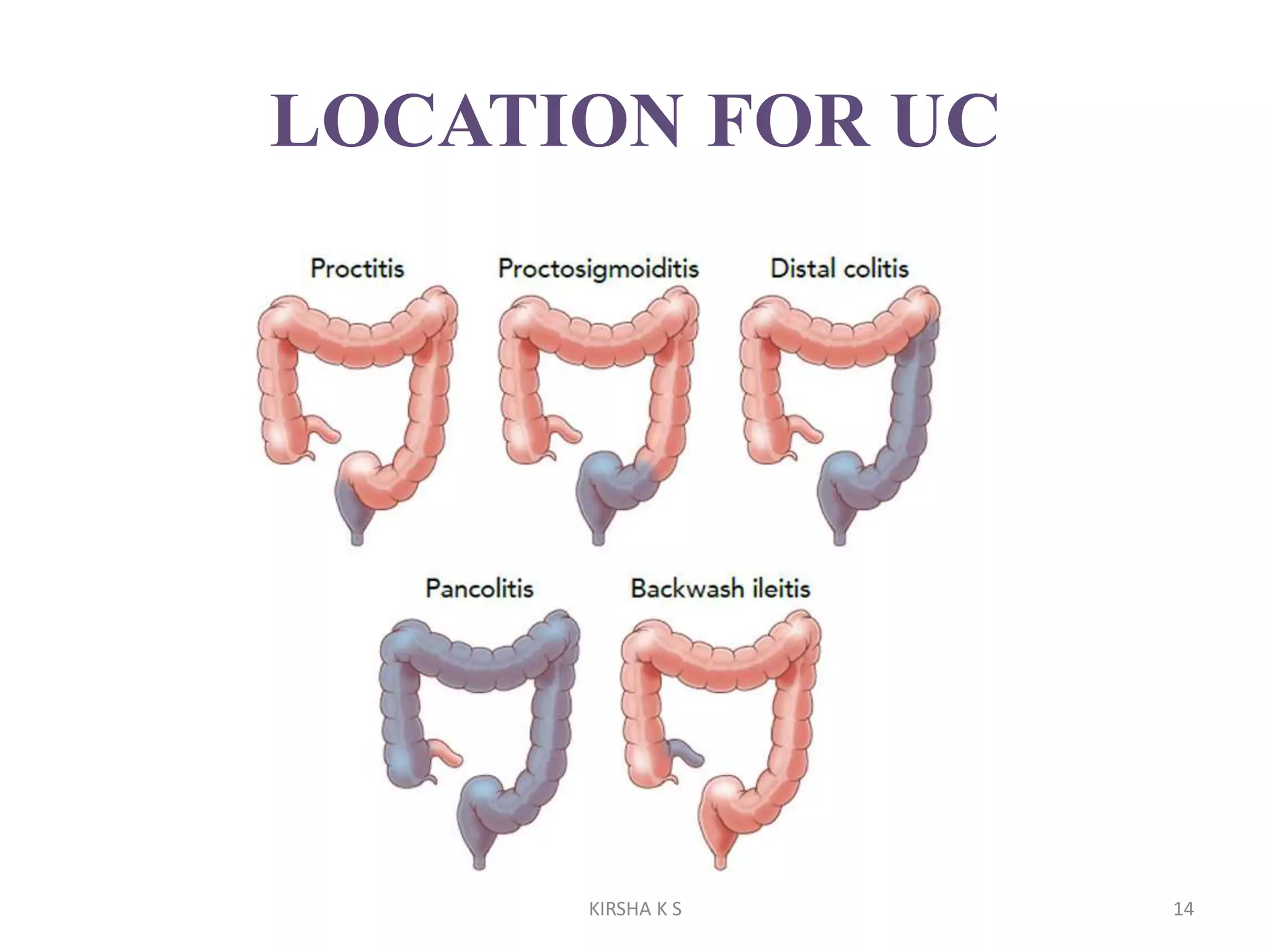
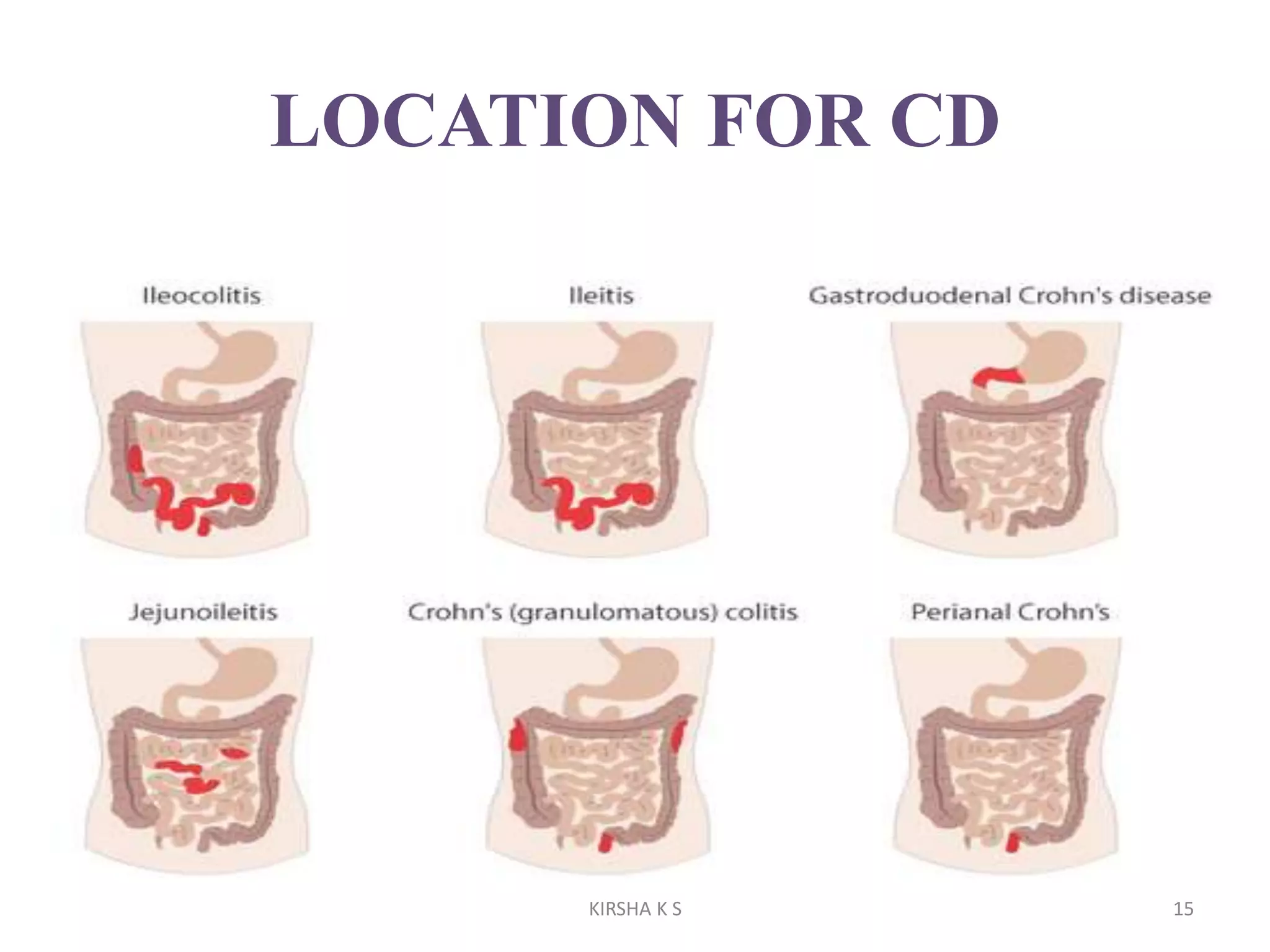

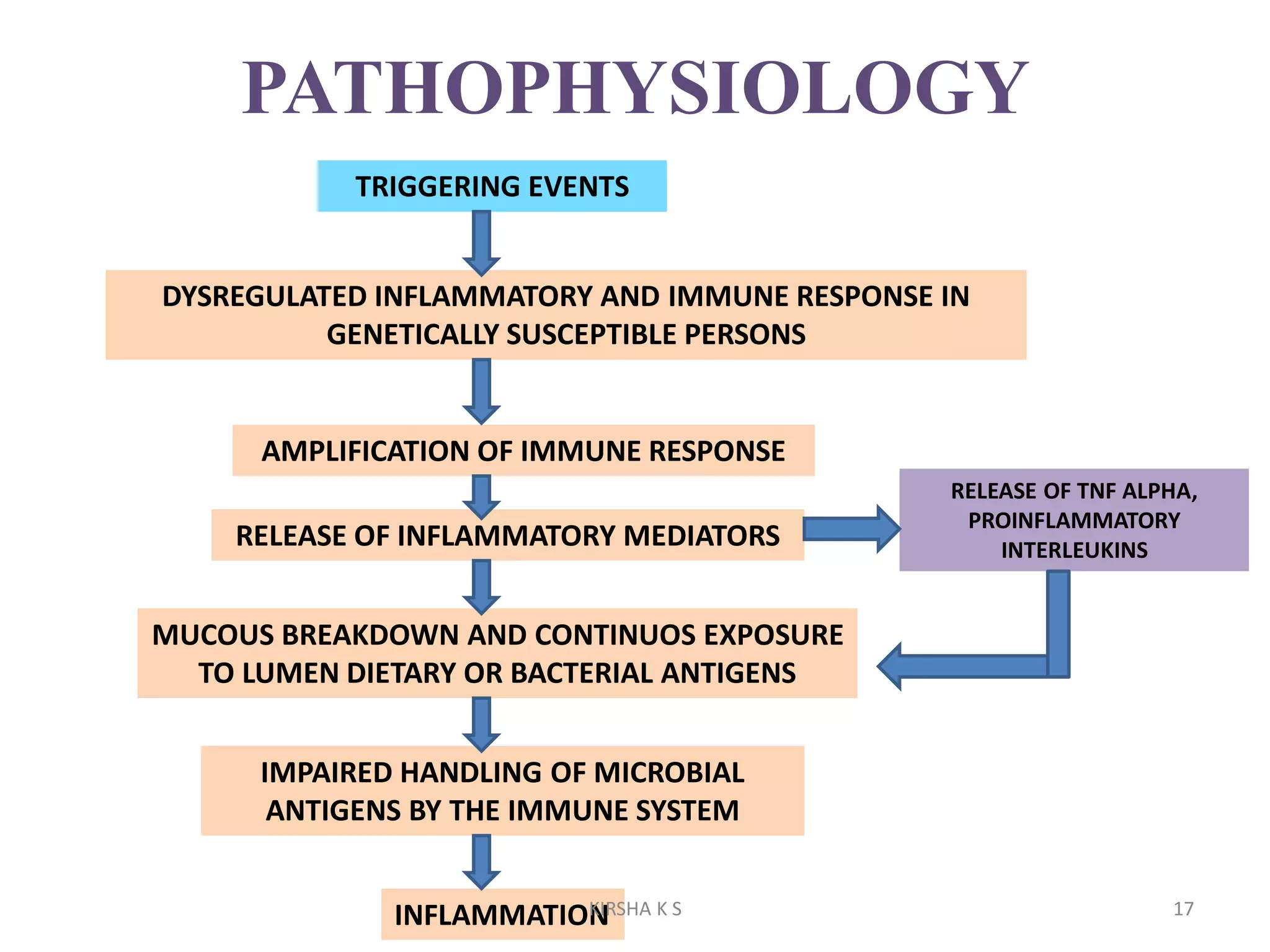
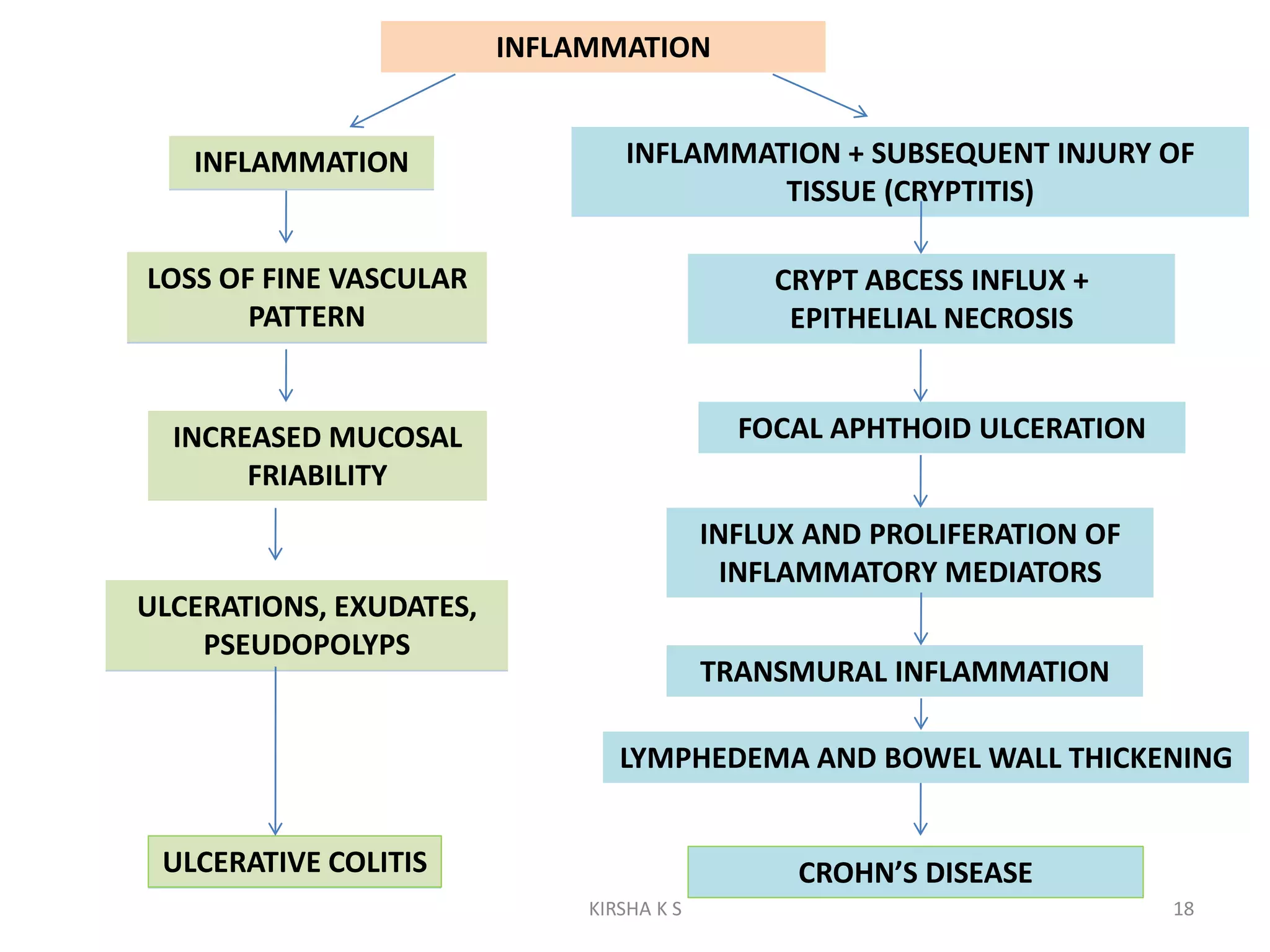
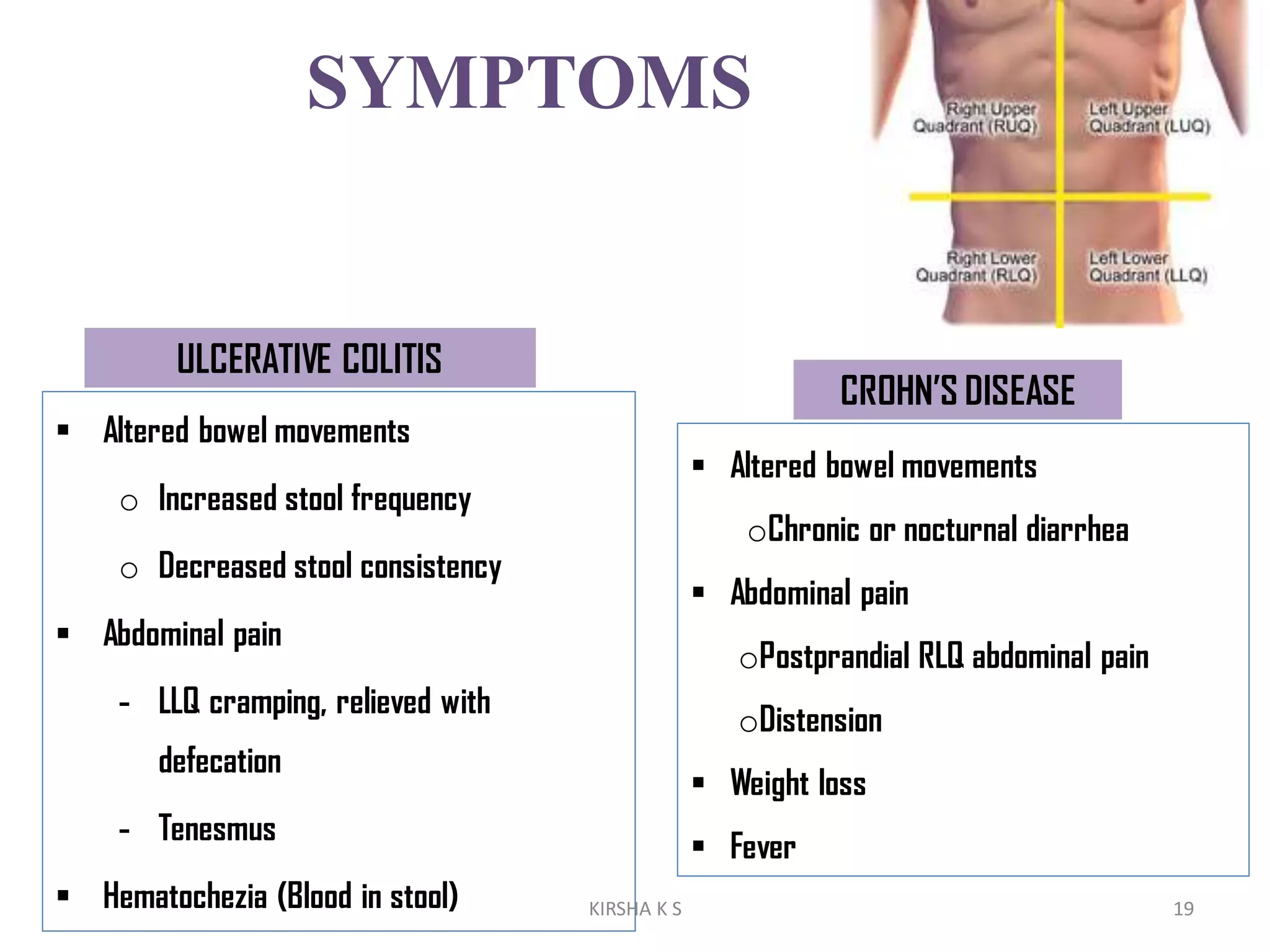
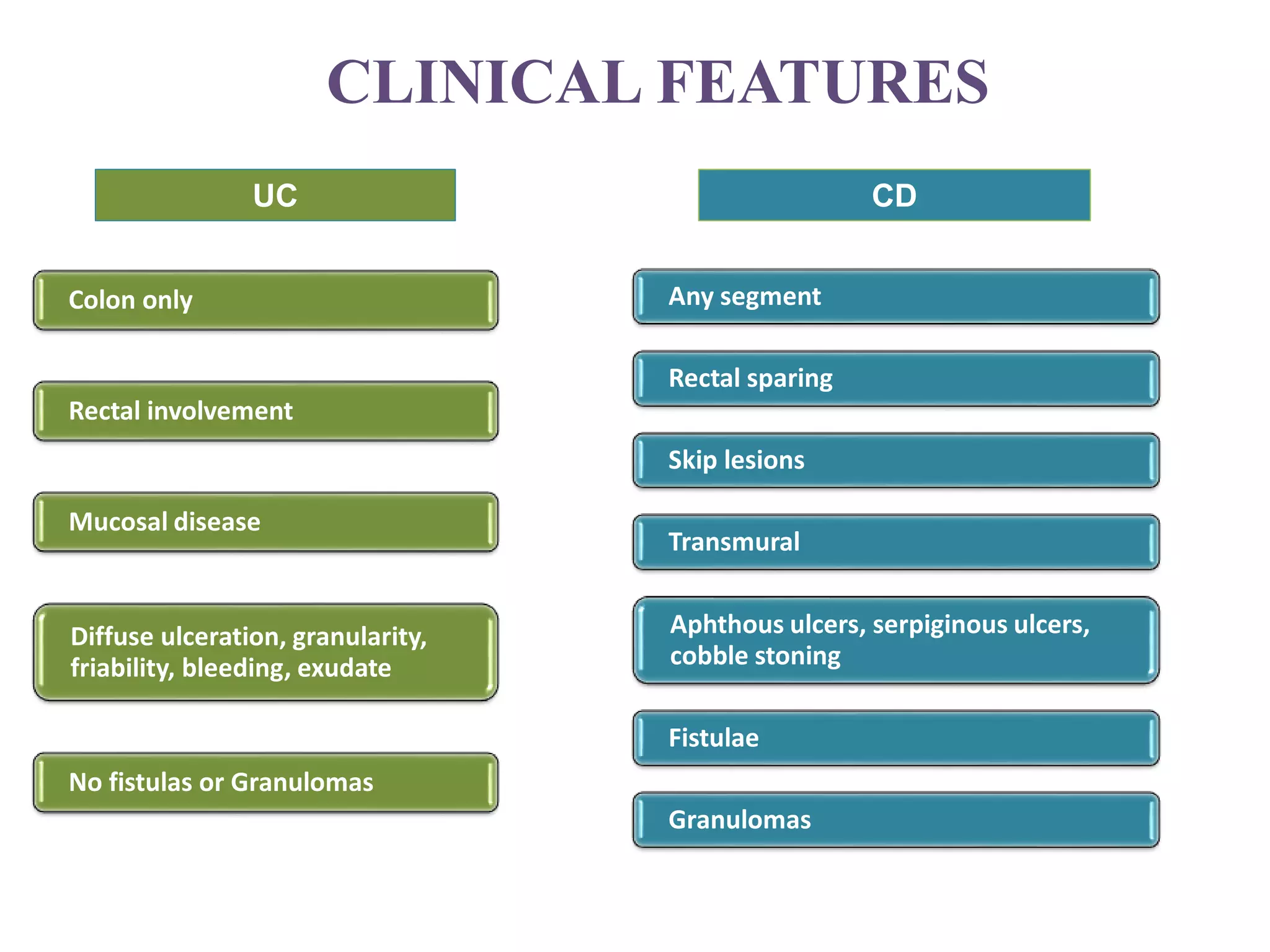
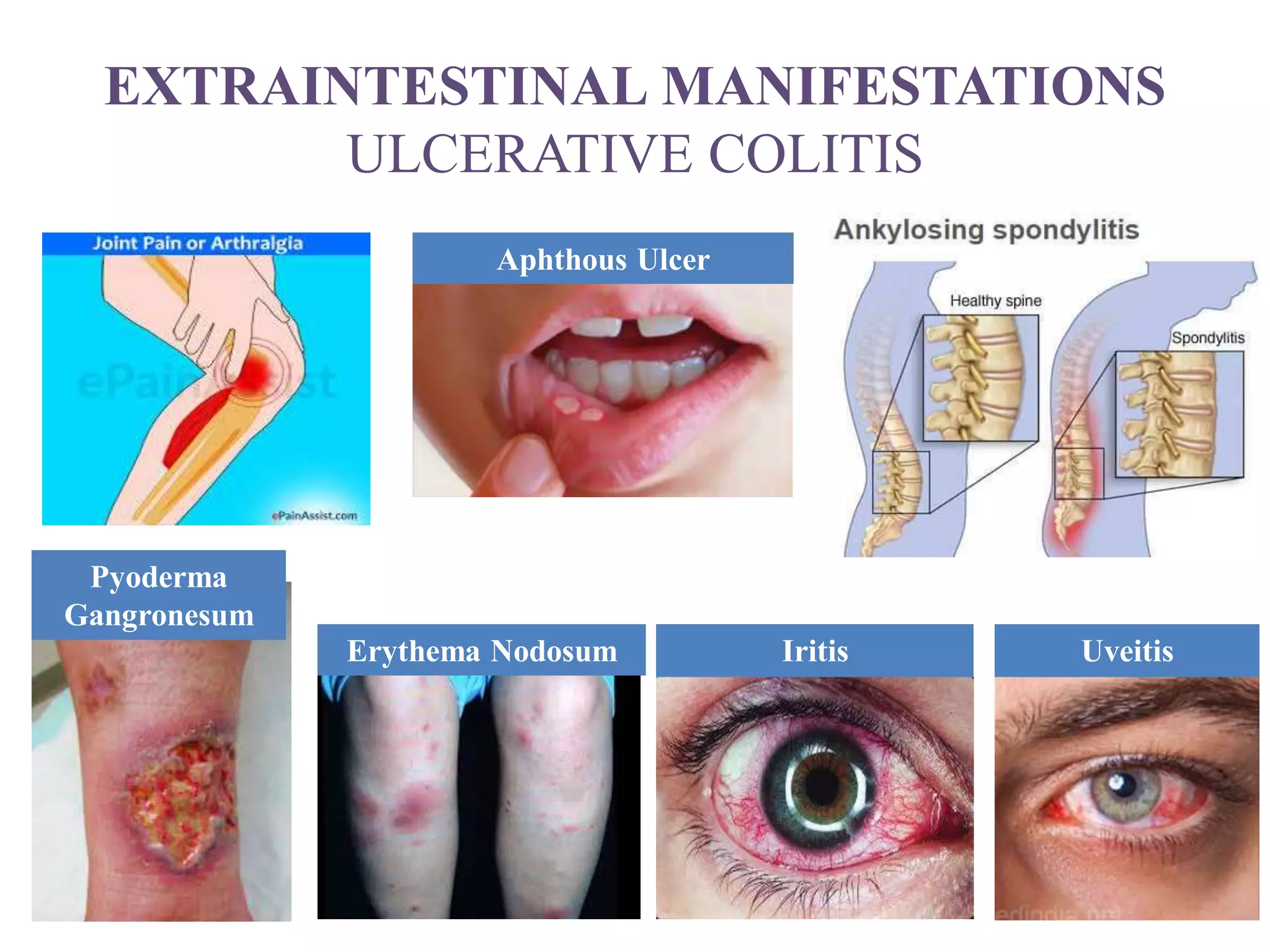
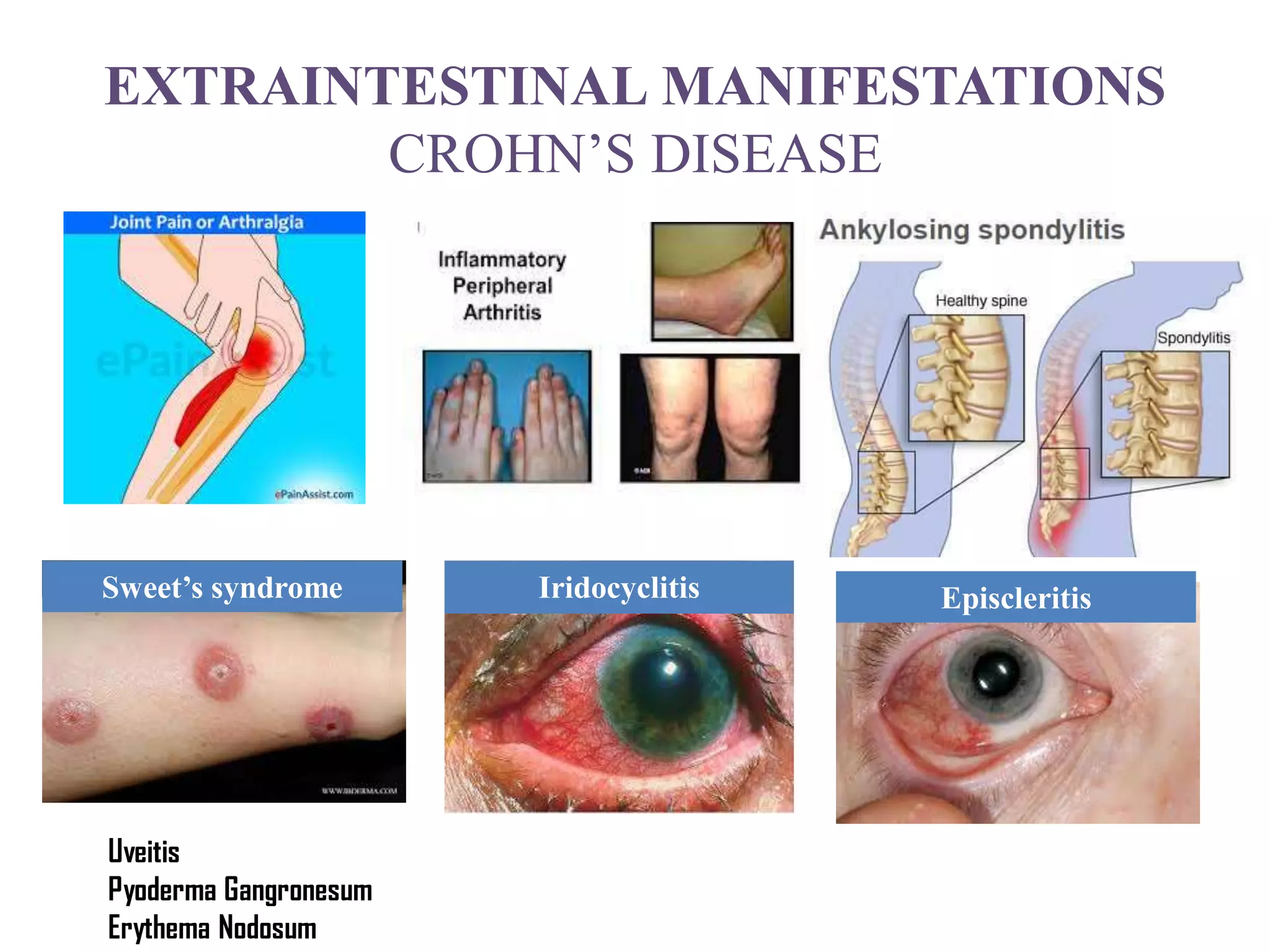





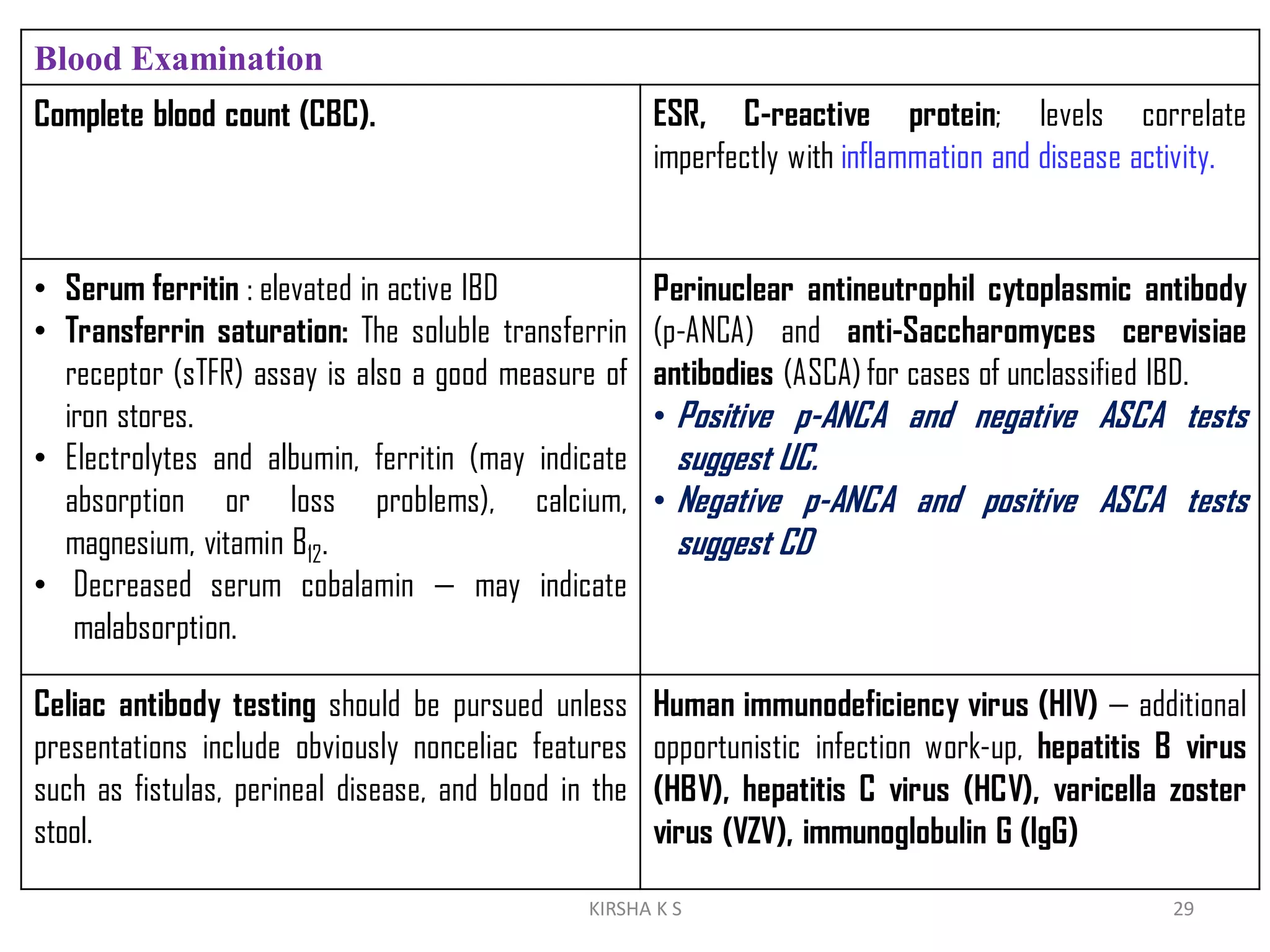
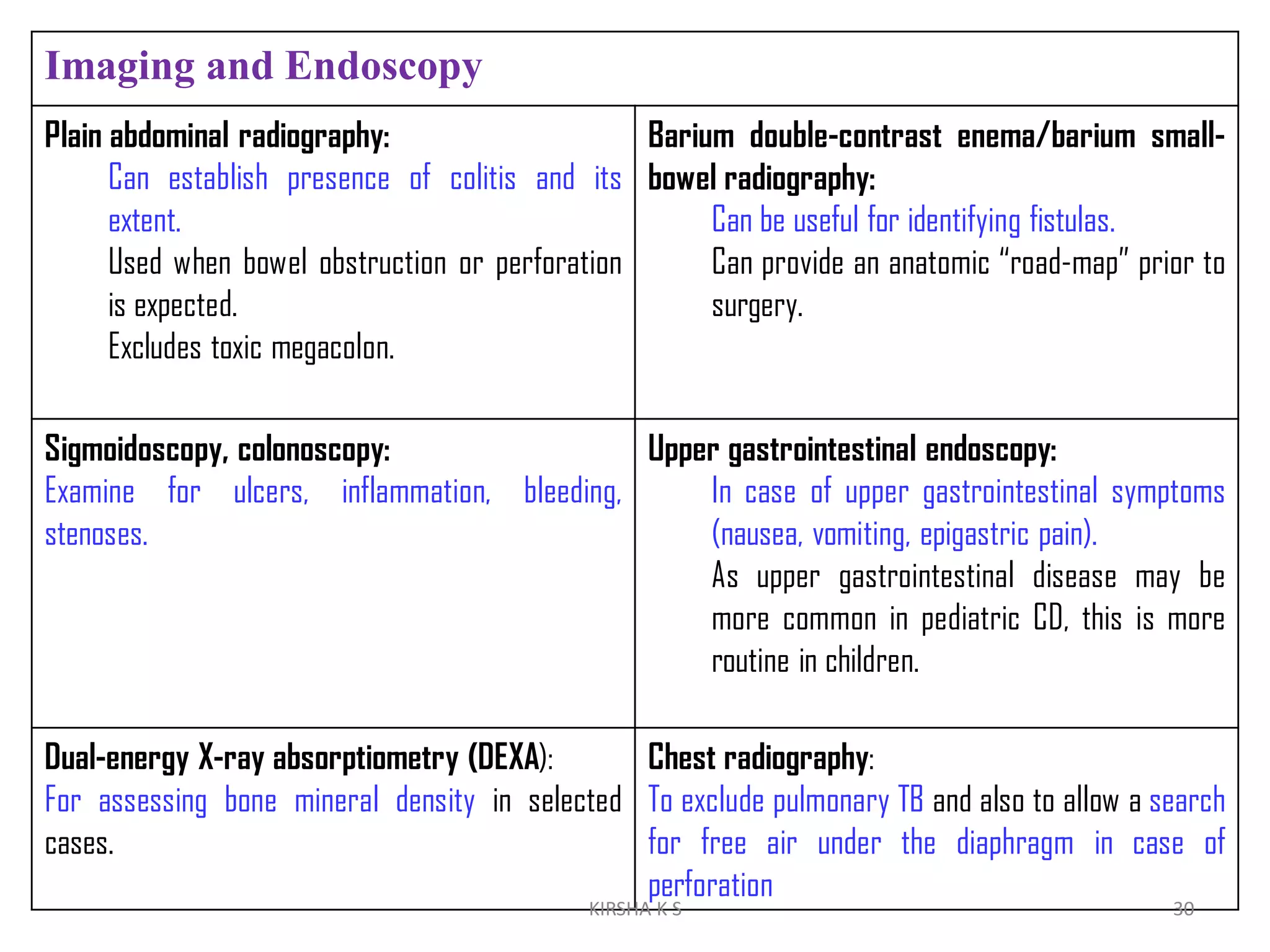
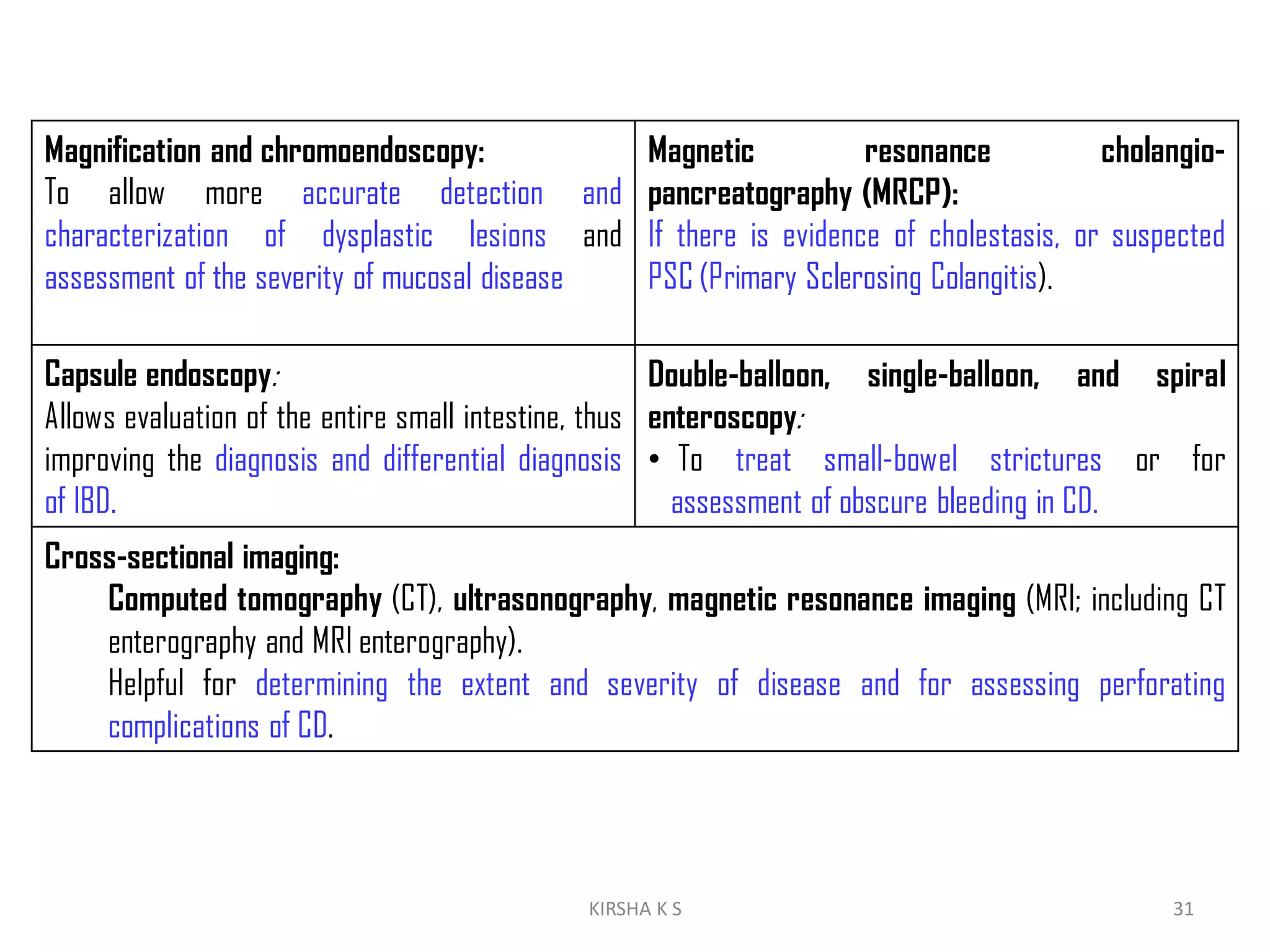
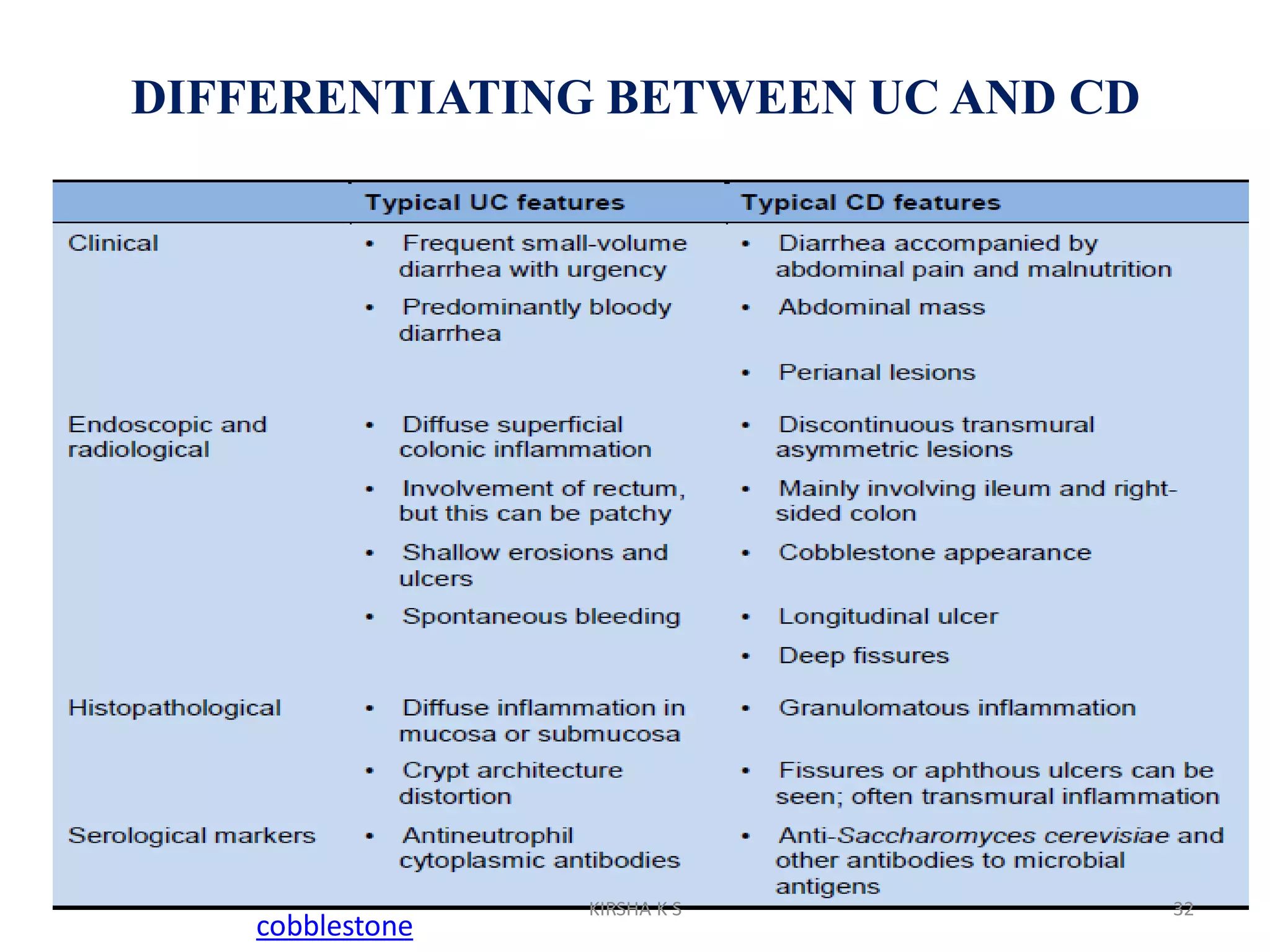














Inflammatory bowel disease (IBD) is a group of chronic inflammatory conditions of the gastrointestinal tract that disrupt the ability to digest food and absorb nutrients. The two main types of IBD are ulcerative colitis, which causes inflammation of the inner lining of the large intestine and rectum, and Crohn's disease, which causes transmural inflammation that may affect any part of the gastrointestinal tract from mouth to anus. Diagnosis involves a review of symptoms, physical examination, blood tests, stool tests, endoscopy, biopsies and imaging studies to determine if inflammation is present and if other causes can be ruled out.



















































































