Download to read offline

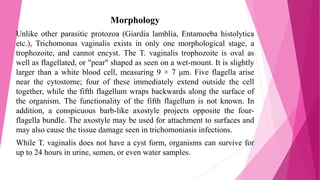
![Mechanism of infection
Trichomonas vaginalis, a parasitic protozoan, is the etiologic agent of trichomoniasis, and is a
sexually transmitted infection. More than 160 million people worldwide are annually infected
by this protozoan.
Symptoms
Trichomoniasis, a sexually transmitted infection of the urogenital tract, is a common cause of
vaginitis in women, while men with this infection can display symptoms of urethritis. 'Frothy',
greenish vaginal discharge with a 'musty' malodorous smell is characteristic.
Signs
Only 2% of women with the infection will have a "strawberry" cervix (colpitis macularis, an
erythematous cervix with pinpoint areas of exudation) or vagina on examination.[8][9][10] This
is due to capillary dilation as a result of the inflammatory response.](https://image.slidesharecdn.com/trichomonasvaginalis-190101152006/85/Trichomonas-vaginalis-3-320.jpg)

Trichomonas vaginalis is a protozoan parasite that causes the most common sexually transmitted infection worldwide, trichomoniasis. It is transmitted through direct skin-to-skin contact, usually during vaginal intercourse. While infections in women often cause symptoms, most infections in men are asymptomatic. An estimated 160 million people are infected annually. Treatment typically involves antibiotics like metronidazole.











































![Report [h.c lab]](https://cdn.slidesharecdn.com/ss_thumbnails/reporth-clab-130125035419-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)











































