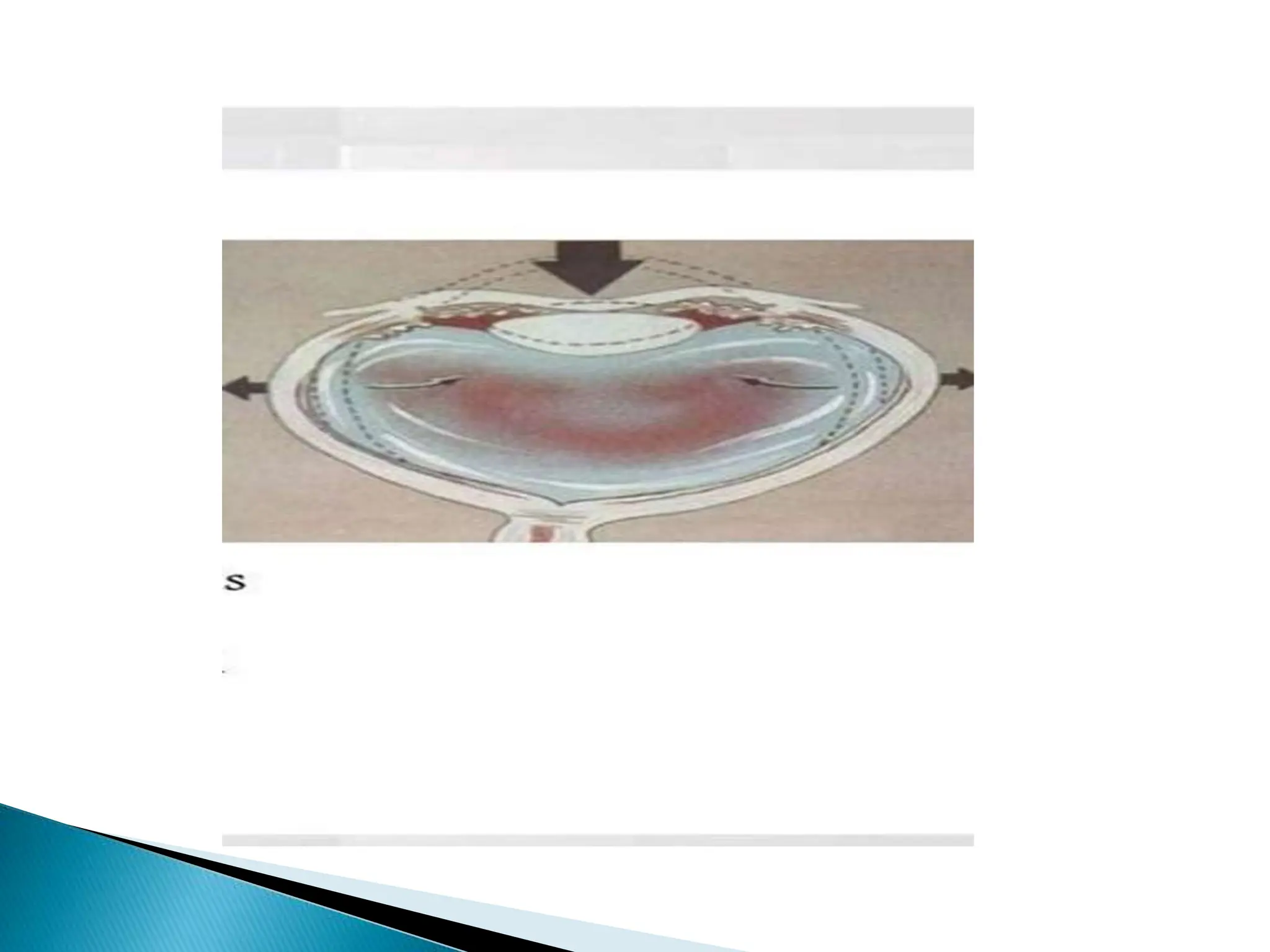
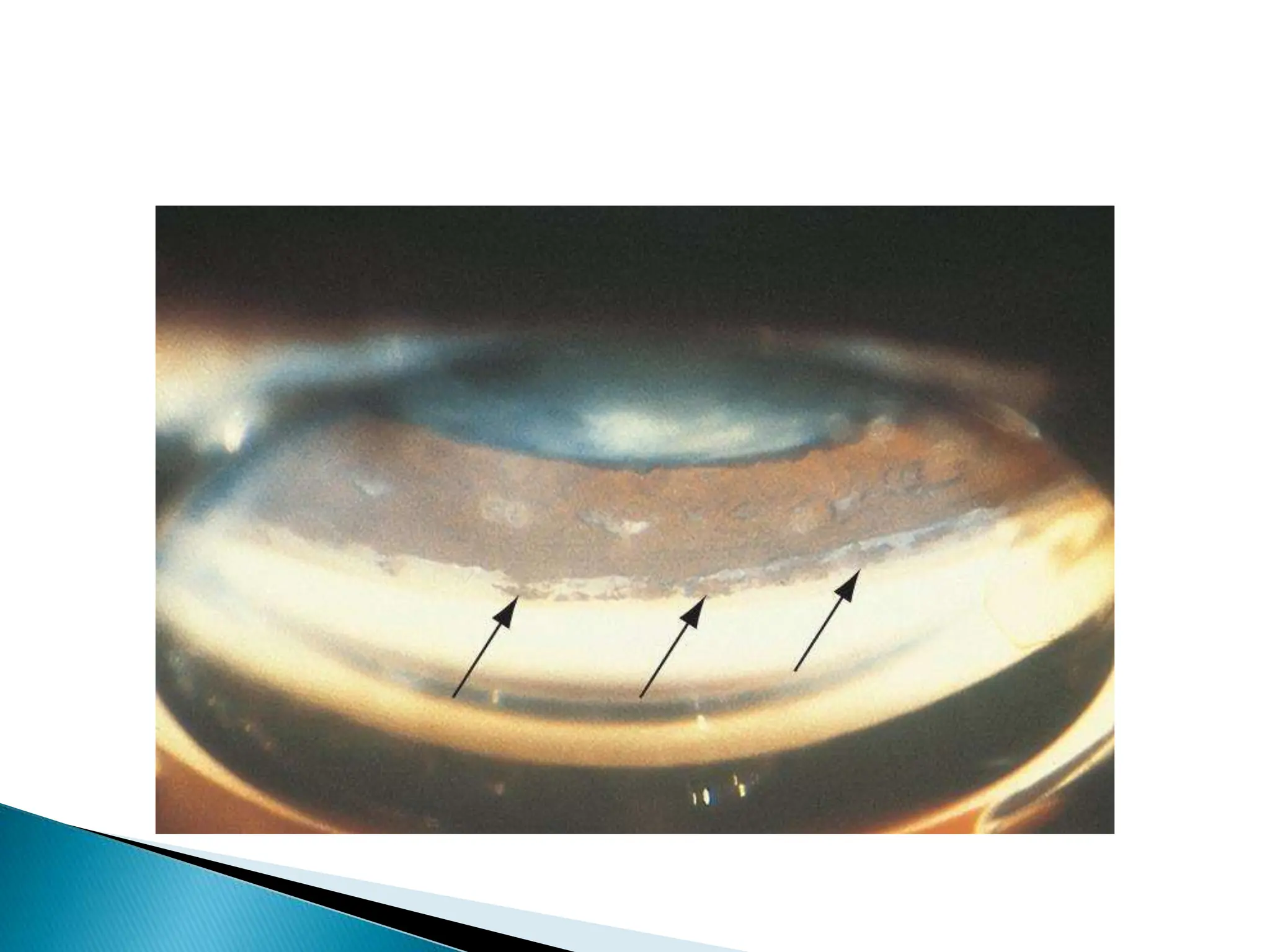
The document discusses lens trauma including subluxation and dislocation. The pathophysiology is described as a compressional force on the eye causing the zonular fibers that anchor the lens to stretch or damage. This can lead to subluxation or complete dislocation of the lens. Clinical findings may include decreased vision, diplopia, myopia, astigmatism, and a tremulous iris. Surgical management depends on the degree of zonular damage and may include lens extraction and intraocular lens implantation. Capsular tension rings can be used to provide circular expansion of the capsular bag and improve stability and centration during surgery.