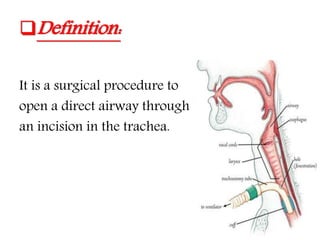
A tracheostomy is a surgical procedure that creates an opening in the trachea to allow direct access to the breathing tube. It is done under general anesthesia with the head extended straight. The incision can be transverse or vertical, depending on whether it is an elective or emergency case. Indications include airway obstruction, impaired breathing function, or assisting with ventilation weaning. Complications can include bleeding, infection, tube issues, or long term stenosis or fistula formation. Decannulation considers when ventilation/suction is no longer needed and the patient can control their airway without risk of aspiration.