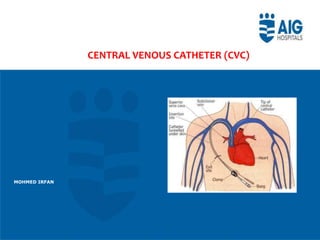
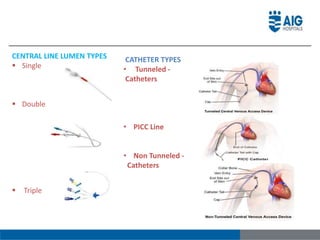
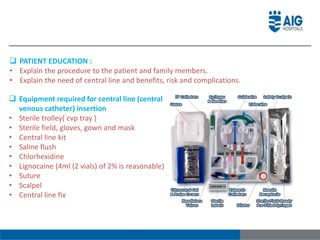
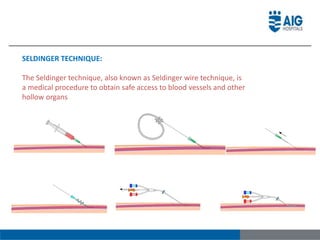
This document provides information on central venous catheters (CVCs). It defines a CVC as a catheter placed in a large vein, with regular sites being the neck, chest, groin, or peripherally. CVCs are used to administer medications, fluids, obtain blood tests, and measure central venous pressure. The document describes CVC lumen types, catheter types including tunneled and non-tunneled, insertion techniques using the Seldinger method, complications, and care/maintenance of CVCs.




























































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)


![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)
![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)





