Downloaded 15 times

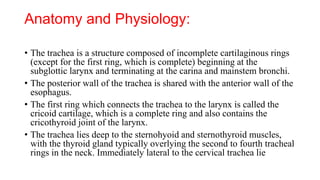













The document discusses tracheostomy, an operative procedure that creates a surgical airway in the cervical trachea, detailing its anatomy, indications, contraindications, techniques, and complications. It outlines various scenarios necessitating tracheostomy, from acute upper airway obstruction to long-term ventilator dependence. Different methods for performing tracheostomy, including open and percutaneous techniques, are compared, highlighting advantages and potential complications related to each approach.