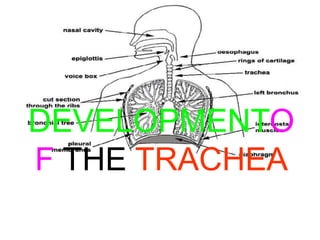
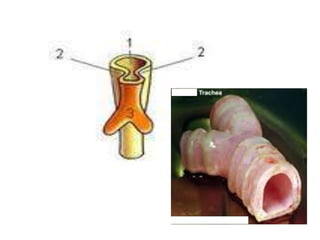
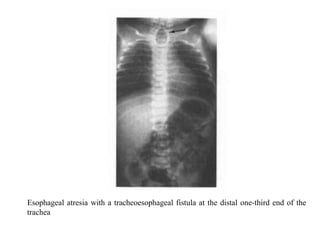
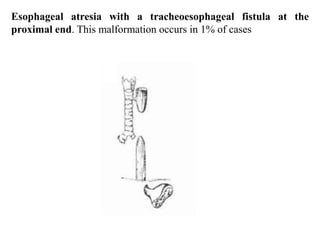
The trachea develops from the endoderm and splanchnic mesoderm. It is a flexible pipe supported by cartilage rings that prevents collapse and allows continued breathing during neck movement. The inner lining contains cilia covered in mucus that traps particles and is pushed toward the mouth and nose, keeping the lungs clean. Tracheoesophageal fistula is an abnormal connection between the trachea and esophagus resulting from improper foregut division, associated with esophageal atresia and polyhydramnios.