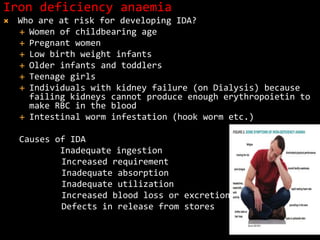
This document discusses essential trace elements in nutrition. It begins by defining trace elements and classifying them as either essential, probably essential, or potentially toxic in low doses. The document then focuses on the essential trace elements iron, iodine, fluoride, zinc, and copper. For each element, it provides details on sources, absorption, functions, deficiency and toxicity symptoms, requirements, and role in oral health. The document emphasizes the critical roles these trace elements play in growth, metabolism, enzyme functions and more.