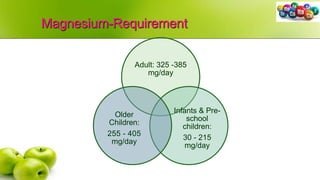
The document discusses the essential roles and functions of various minerals in human nutrition, categorized into major and trace minerals. It explains their importance in physiological functions, sources, daily requirements, and associated disorders like deficiencies and excesses. Key minerals highlighted include calcium, phosphorus, magnesium, sodium, potassium, iron, iodine, copper, and zinc, detailing their functions in bone health, enzyme activity, and metabolic processes.







![Iodine-Sources
• The best sources of iodine are sea foods (e.g., sea fish, sea salt)
and cod liver oil
• Smaller amounts occur in other foods, e.g., milk, meat, vegetables,
cereals, etc.
• The iodine content of fresh water is small & very variable, about 1-
50 micrograms/L
• About 90 per cent of iodine comes from foods eaten; the remainder
from drinking water.
• Fortified Salts— Iodized salts (prophylactic) [iodized bread, iodized
oil]
• 50 ppm at production level
• 30 ppm in retailer level
• 15 ppm at consumer level](https://image.slidesharecdn.com/g0yqjar0reclovbkqnle-signature-5b9bc7e82fbff7c04e6dde2c05d063a1abe0044e1da7a8d56655b744cce3a9cc-poli-210605134958/85/Minerals-in-Food-36-320.jpg)