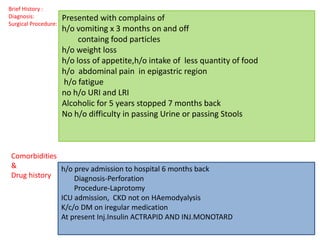
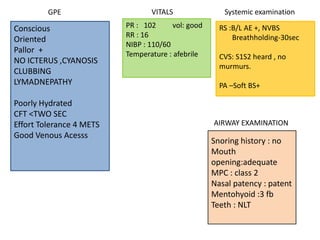
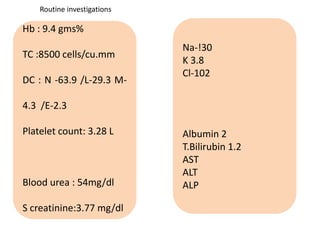
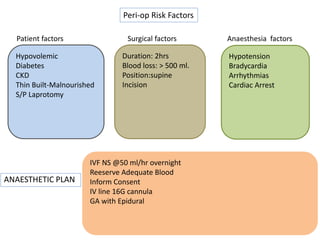
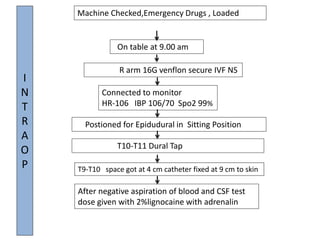
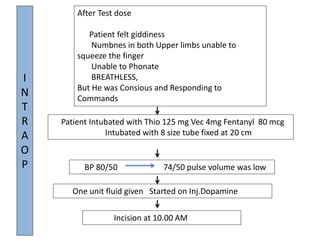
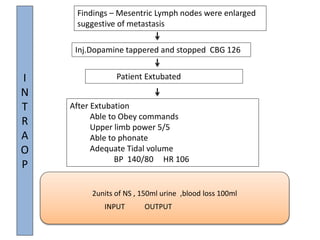
This document summarizes a patient's medical history and details of a surgical procedure under anesthesia. A 45-year old male patient presented with vomiting, weight loss, abdominal pain and fatigue. He had a history of perforation and laparotomy surgery. The patient was diagnosed with CKD and diabetes. He underwent a total spinal anesthesia for a 2-hour surgery to investigate enlarged mesenteric lymph nodes. During the procedure, the patient experienced hypotension and bradycardia due to the spinal anesthesia. He was intubated and given intravenous fluids and medications to stabilize him. After the surgery, the patient was extubated and able to follow commands with normal vital signs.
































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















