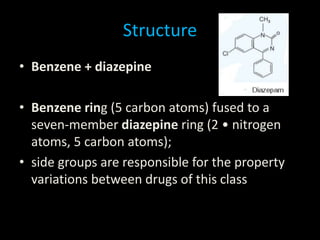
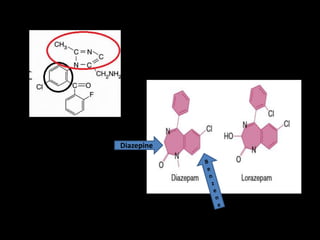
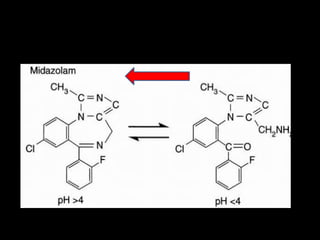
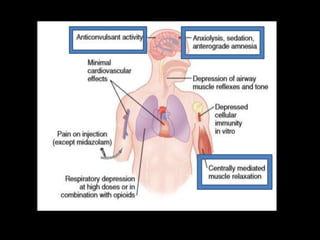
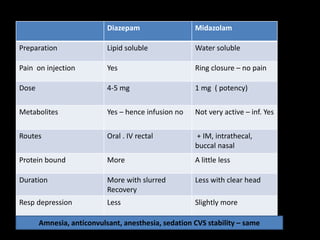
Benzodiazepines are a class of drugs that enhance the effects of the neurotransmitter GABA at GABA-A receptors in the brain, producing anxiolysis, sedation, anticonvulsant effects, muscle relaxation and amnesia. Common benzodiazepines include diazepam, midazolam and lorazepam. They are used for premedication, anesthesia, sedation, status epilepticus and withdrawal symptoms. While effective, they can cause side effects like fatigue, drowsiness, impaired cognition and paradoxical reactions with prolonged use.





















































![4._Sedative_hypnotics[1].pptx pharmacy students](https://cdn.slidesharecdn.com/ss_thumbnails/4-251117163021-acac7ad2-thumbnail.jpg?width=640&height=640&fit=bounds)
































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






