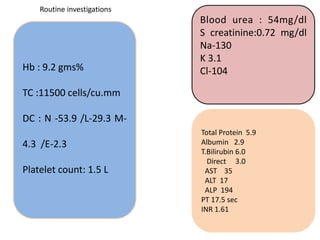
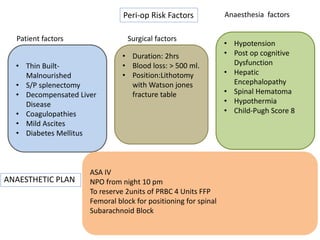
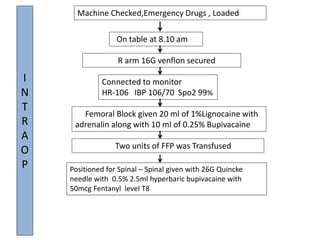
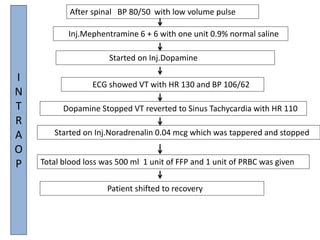
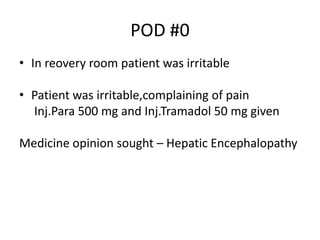
This document summarizes a 39-year-old male patient who presented with an intertrochanteric fracture of the left hip. He had a history of diabetes, liver disease, splenectomy, and alcohol use. He underwent a closed reduction and internal fixation with a proximal femoral nail. The anesthetic plan addressed his comorbidities and perioperative risks. Intraoperatively, he developed ventricular tachycardia which resolved with medication. He received blood products due to blood loss. Postoperatively, he showed signs of hepatic encephalopathy.


































![[Nini] General Surgery - Case Presentation.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ninigeneralsurgery-casepresentation-260104220312-c8c97998-thumbnail.jpg?width=640&height=640&fit=bounds)















































