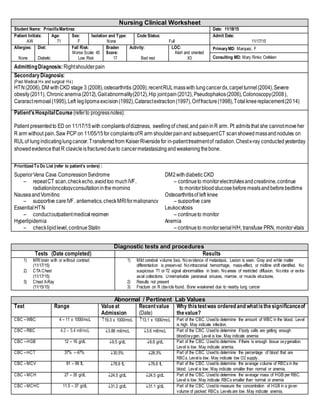
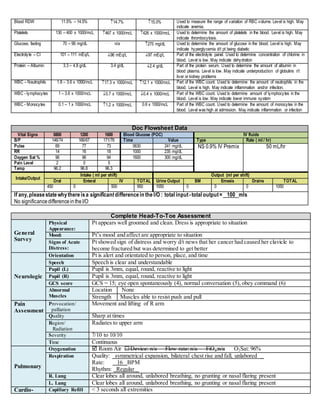
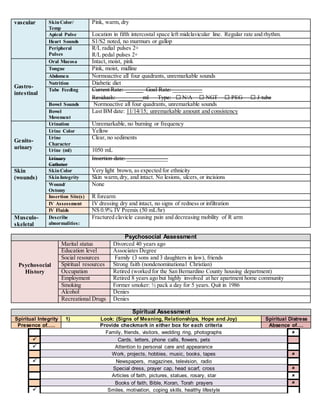
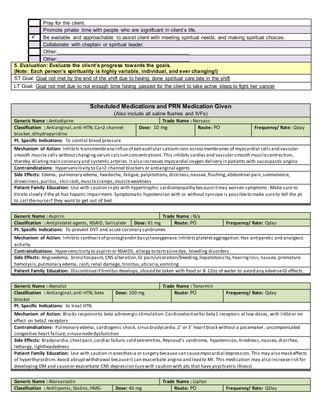
This document provides a comprehensive care plan for a 71-year-old female patient admitted for right shoulder pain. She has a history of multiple medical issues including lung cancer, diabetes, and hypertension. On admission, she was found to have a fractured right clavicle due to cancer metastasis. Lab work showed abnormalities including anemia. The plan identifies interventions to address issues such as spiritual distress, diabetes management, and pain control. Goals are set to improve spiritual well-being and engage in cancer treatment. Nursing will provide support, hope, and a therapeutic relationship.






































![[20170101][Case Presentation][Internal Medicine][Chen, Chia Ching]](https://cdn.slidesharecdn.com/ss_thumbnails/20160101casepresentationinternalmedicinechenchia-ching-171114231129-thumbnail.jpg?width=640&height=640&fit=bounds)










