Case Presentation -TURP
Moderator - Dr Pinu Ranawat Mam/Dr Jahanvi Mam
Presented by - Dr Vivek
2.
TURP - INTRODUCTION-
• Gold standard surgical treatment for benign prostatic hyperplasia (BPH).
• Location - Just below bladder surrounding urethra.
• Normal weight - 20-30 g
• Performed in patients prostate weight > 60 g
• Involves resection of prostatic tissue by bipolar electrocautery with diathermy
loop ( at end of urethroscope ) which can both cut and coagulate.
• Urethroscope is inserted into patient urethra & tissue is resected into small pieces.
• Bladder is continuously irrigated with fluid to clear blood & debris by a three
lumen catheter.
• Irrigation fluid continued for 24 hr after OT.
• Procedure takes 30-90 min.
• Procedure is performed in lithotomy position.
3.
A 65 yearsold man with benign prostatic
hypertrophy scheduled for transurethral
resection of prostate.
4.
HISTORY -
Nathu ,65 year old male, Resident of village kherwara, Udaipur, farmer
by occupation, belonging to lower middle class , presented with chief
complaints of -
- Dysuria ( painful urination with burning sensation ) 1 month
- Urgency ( sudden need to urinate , not able to control urine ) 1 month
- Hesitancy ( difficulty in starting urination with a weak urine stream )
- Right flank pain 1 month
- Retention of urine since 1 month
- Gross hematuria since 3 months
- Increased frequency of micturition since 6 months
- Dribbling of urine during micturition since 6 months
- Feeling of incomplete bladder emptying since 6 months
5.
HOPI -
Patient wasapparently well 6 months ago, when he noticed increased frequency of micturition,
with waking up at night multiple times for voiding, leading to sleep disturbances. He also gave
history of dribbling of urine with weak urine stream during micturition, along with difficulty in
starting of micturition, which was gradually progressive, since 6 months. He also had a sense of
incomplete bladder emptying post micturition. 3 months ago, he complained of gross hematuria
while micturition, associated with pain lower abdomen, burning micturition.
No h/o significant weight loss or loss of appetite.
No h/o fever, vomiting.
No h/o previous catheterization.
No h/o IHD, dyslipidemia, CVA, malignancy.
No h/o bronchial asthma, thyroid.
6.
Past History -
-Patient had history of anemia (due to gross hematuria- Hb 8.3 g/dl), for
which 1 unit PRBC was transfused on 25th december 2025, along with
supplementation of iron and folic acid orally.
- Patient is not a known case of HTN , DM, Bronchial Asthma,
Pulmonary Tuberculosis , Epilepsy, Ischemic heart disease.
- No H/o past surgery
7.
PERSONAL HISTORY-
- Heconsumes mixed diet. He has disturbed sleep due to awakening to pass
urine. His bowel habits are normal.
- Non smoker and non alcoholic.
- Family history - Not significant
8.
GENERAL PHYSICAL EXAMINATION-
- Patient is comfortable in sitting as well as supine position . Conscious and
oriented to time, place and person.
- No pallor, icterus, cyanosis, clubbing, lymphadenopathy, edema.
- Patient is afebrile
- PR- 88 bpm, regular in rate, rhythm, normal in volume
- BP- 122/70 mmHg in right brachial artery in sitting position
- SpO2 – 97% on room air
9.
INSPECTION - Abdomenis not distended. Umbilicus central in position , All
quadrants are equally moving with respiration.
PALPATION - No organomegaly, no mass per abdomen
PERCUSSION - Tympanic note all over the abdomen
AUSCULTATION - Bowel sounds present.
EXAMINATION OF ABDOMEN -
10.
Per rectal examination-
- No fissure , No external hemorrhoids
- Sphincter tone normal
- Enlarged prostate gland is felt against anterior abdominal wall
Respiratory examination -
- Auscultation: B/L Normal air entry with no added sound
- Palpation: No swelling or tenderness
- Equal expansion of chest during respiration
- Trachea central in position
- Percussion: Normal
11.
Cardiovascular Examination -
-Inspection: No enlargement of neck veins, no visible pulsations
- Palpation: Non tender, Cardiac impulse in 5th ICS, medial to
midclavicular line
- Auscultation: S1 S2 Normal. No added sounds
Central nervous system -
- Muscle built, tone, power, co-ordination - WNL in all 4 limbs
- All sensory functions and reflexes are intact
- Gait is normal
- Vertebral column - No deformity, no sacral edema & non tender
12.
Airway Examination -
-Mouth Opening - 3 finger
- Mallampati Score – Grade II
- Neck Movement – adequate
- Thyromental Distance - > 6.5 cm
- No loose / artificial tooth
13.
DIAGNOSIS -
65 yearold male patient ,with complaints of increased frequency of urine,
dribbling of urine , sense of incomplete bladder emptying is probably a
case of benign prostatic hyperplasia posted forTURP
Pre-op Prepartion -
-NBM after midnight
- Optimization of pre-existing co-morbid conditions
- Tab Alprazolam 0.25 mg OD HS
- Tab Ranitidine 150 mg OD 6 AM
- Antibiotic prophylaxis (in case of urinary tract infection )
- Arrangement of blood and blood products
- Fresh written informed consent
16.
OT Preparation -
-Fluid warmer
- Ambient OT temperature
- Emergency drugs
- Airway equipments
- Suction
17.
Monitoring -
- ECG
-Pulse-oximeter
- NIBP
- Temperature probe
- Mental activity
- Blood loss
- S. electrolytes
- EtCO2 if GA is used
18.
PREANESTHETIC ASSESSMENT -
•To see co-morbidities - HTN ,DM, IHD, Renal Dysfunction
• To see on medications - Blood thinner ( aspirin) , oral anticoagulants (warfarin , dabigatran ,
rivaroxabin )
• Age related organ changes are :-
Central nervous system -
- Reduced functional tissue in CNS is one of the major factor that reduces anesthetic doses in
older patients.
- Older patients have - sluggish , impaired , absent reflexes responses which may complicate
monitoring.
19.
• Loss offunction of special senses such as sight , hearing leads to apprehension
and sometimes sedation is needed to reduce pre-operative stress which can
increase sympathetic stimulation.
• Geriatric population has reduced ability to generate body temperature which is
more susceptible to develop hypothermia during prolonged surgery & post op.
• Super sensitivity of post synaptic receptors may prolong action of muscle
relaxants .
20.
Cardiovascular System -
•Impaired cardiovascular function should be expected in elderly patients.
• Baroreceptor function may be impaired in patients with Congestive heart
failure & cardiovascular system to compensate surgical hemorrhage for
vasodilatory effects of anesthetic agents results in hypotension.
• Anesthetic agents depress cardiac function & cardiac arrest can be
identified if cardiac arrhythmias present particularly ventricular
arrhythmias , right bundle branch block or bradycardia.
• Monitoring HR , BP , Pulse is important during anesthesia.
21.
Respiratory system -
•Age relate degenerative changes decreases pulmonary function
• Reduced alveolar surface area
• Reduced diffusion capacity
• Reduced lung elasticity
• Reduced mechanical ventilation reserve
• Pulmonary embolism is common post-op complication in older
patients.
22.
Renal -
• Impairedrenal function, prolong plasma half life of drug elimination
via kidney which alters the fluid , electrolytes , acid base balance.
• If hypotension , occurs during anesthesia tubular ischemia occurs
which results in acute tubular necrosis & renal failure.
• Advancing age & general anesthesia are important risk factor for
development of renal failure.
23.
Liver -
• Inimapired hepatic function, plasma clearance rate for drug decreases
which results in increses duration of action.
• In humans , Bromosulphalein retention increses with age.
• Bromosulphalein - Red dye , used in liver function tests , taken up by
hepatocytes excreted in bile , rapid clearance from blood stream shows
healthy liver function , prolonged retention in blood after a set time
shows impaired liver functions.
24.
CHOICE OF ANAESTHESIA-
• Regional anaesthesia is the technique of choice for TURP.
• TECHNIQUES:
• Subarachnoid block - is preferred
• Epidural block
• Caudal block
• Saddle block
• Level of sensory block -
- T10 dermatome level – to eliminate discomfort caused by bladder
distention
- T9 dermatome level – enable to see capsular sign (pain on
perforation of prostatic capsule)
25.
CHOICE OF ANAESTHESIA-
- Patient taken on OT table
- Standard monitoring attached.
- SpO2 – 97%, NIBP – 127/84 mm Hg, HR – 92 / min, ECG - WNL
- IV line secured with IV cannula 18 G on right hand, Intravenous fluids started
- Spinal Anesthesia is given with 2.6 ml of 0.5% hyperbaric bupivacaine
- Level of Spinal Anesthesia is maintained to T10
- Disadvantage - Hypotension
26.
Advantages of regionalanesthesia -
- Allows monitoring of mental status and early signs of TURP Syndrome.
- Detection of bladder perforation.
- Promotes peripheral vasodilatation and reduces circulatory overload.
- Reduces blood loss, requiring fewer blood transfusions.
- Good postoperative analgesia.
- Neuroendocrine and immune responses are better preserved.
- Lower cost
27.
GENERAL ANAESTHESIA -
ADVANTAGES-
• Useful for patients who are unable to lie supine.
• Useful for patients with neuromuscular diseases and pulmonary
compromise.
DISADVANTAGES -
• Unable to monitor mental status.
• Possibility of difficult airway and risk of aspiration.
• Reduced FRC due to lithotomy position.
• Postoperative nausea and vomiting.
• Postoperative analgesia needed.
28.
EPIDURAL ANAESTHESIA -
BENEFITSOF EPIDURAL ANESTHESIA -
• Ability to titrate the drug to the effective level of sensory block.
• Help reduce chronic pain levels.
• Intra-operative anaesthesia and postoperative analgesia.
• Less respiratory depression.
• Less hemodynamic instability.
• Less incidence of higher block.
29.
Characteristics of idealirrigation fluid -
1.Transparent
2. Isotonic
3. Non electrolytic
4. Non haemolytic
5. Inexpensive
6. Not metabolizable
7. Rapidly excreatable
8. Non toxic
32.
Factors affecting rateof absorption of fluid-
RULE OF 60 -
• Duration of surgery- 60 minutes
• Age of patient- more than 60 years
• Size of prostate gland - more than 60 grams
• Height of irrigation fluid- 60cm above pubic symphysis
• Hydrostatic pressure- 60 cm of H20
• Integrity of prostatic capsule
CONCERNS OF LITHOTOMYPOSITION -
• Lithotomy position first consideration - is to fit the equipment to patient not the patient to
equipment.
• Lithotomy position - Supine on table , patient legs elevated together flexed together put in
stir rups , thighs are flexed at about 90 ′ to abdomen & outward rotated.
Complications with lithotomy position :
• Injury to peripheral nerves - Common peroneal, posterior tibial, lateral femoral cutaneous
nerve, saphenous nerve, obturator nerve, sciatic nerve
• Venous stasis - Occurs in prolonged lithotomy position , stasis occurs at point of
compression by equipment or at groin region due to thigh flexion.
- patients with varicose veins are at high risk
• Preventive measure - If lithotomy position > 15 min , legs have to be protected by elastic
stockings.
• Stress on lumbar spine - lower back pain
35.
Primary concern ofturp -
• Intravascular absorption of large volume of irrigation fluid during
procedure.
• Absorption occurs by exposed venous sinuses of surgical capsule.
• Hypoosmolality is more important than hyponatremia in causing CNS
disturbances.
36.
COMPLICATIONS OF TURP-
INTRAOPERATIVE COMPLICATIONS -
• TURP Syndrome
• Hypothermia - due to use of cold irrigation fluids.
• Myocardial Infarction
• Bleeding and bladder perforation
POSTOPERATIVE COMPLICATIONS -
• TURP Syndrome
• Clot retention
• Bleeding and disseminated intravascular coagulation (DIC)
• Postoperative Cognitive Dysfunction
37.
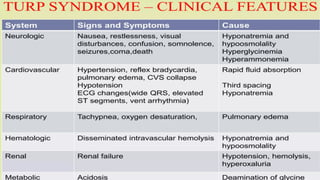
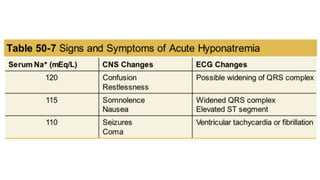
TURP SYNDROME -
•It is a constellation of symptoms & signs caused by absorption of irrigating
fluids.
Pathological Triad - Hypervolemia, Hypoosmolality, Hyponatremia
Symptoms -
• Clinical Triad - Hypertension, Bradycardia, Mental Changes
• CNS manifestations - Disorientation, restlessness, confusion,
drowsiness ,convulsions and coma.
• CVS manifestations - Dyspnoea, pulmonary congestion, pulmonary oedema,
and cardiac overload. Due to fluid overload and the negative ionotropic effect of
hyponatremia.
• Haemolysis
• Hypothermia
40.
Factors affecting amountand rate of fluid absorption -
- Size of gland (25ml/gm of prostate)
- Number and size of open sinuses
- Hydrostatic pressure of irrigating fluid
- Duration of procedure @ 20-30 ml/min
- Integrity of capsule
- Venous pressure at irrigant-blood interface
- Vascularity of diseased prostate
41.
MANAGEMENT -
1. Administer100% oxygen.
2. Ask surgeon to stop the surgery.
3. Airway, breathing, circulation.
4. Management of hyponatremia -
• Treat mild symptoms (with serum Na+ concentration >120 mEq/L) with fluid
restriction and loop diuretic (furosemide)
• Treat severe symptoms (if serum Na+ <120 mEq/L) with 3% sodium chloride
IV at a rate <100 mL/hr
• Discontinue 3% sodium chloride when serum Na+ >120 mEq/L
42.
Bladder Perforation -
Intraperitonealor Extraperitoneal -
• Signs & symptoms:
- Abdominal distension
- Suprapubic pain radiating to shoulder
- Rigidity
- Autonomic signs like pallor, nausea, vomiting, diaphoresis
- Bradycardia, Hypertension
- Non return of irrigating fluid
Treatment:
1. Localized, extra peritoneal- Catheterization and antibiotics
2. Intraperitoneal- Surgical exploration, drainage and repair
43.
POST OP CONSIDERATIONS-
Monitoring for TURP syndrome - Can develop upto 24 hours.
• Serial monitoring of Na+, K+, Ca2+, ABG, Coagulation profile,
osmolarity.
• Postoperative Cognitive dysfunction
• Postoperative analgesia

















































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)










