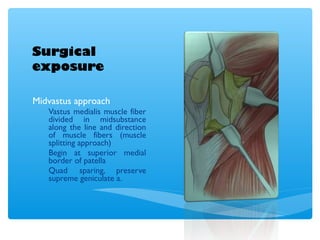
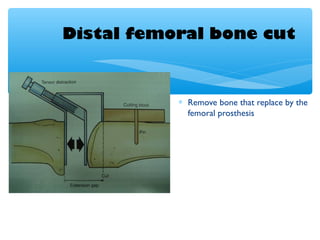
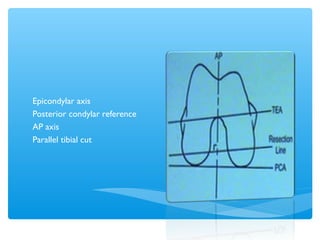
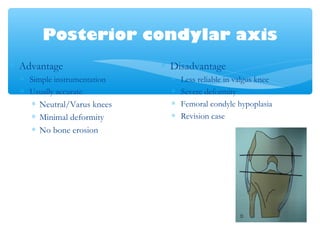
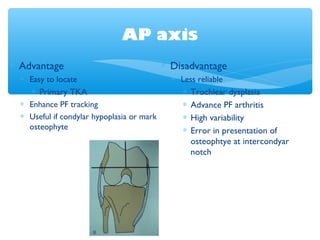
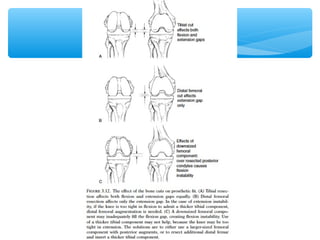
This document discusses the evolution and design of total knee arthroplasty (TKA). It describes how early TKA designs in the 1970s-1980s led to improved designs that better replicated normal knee biomechanics. The key developments included posterior cruciate ligament retaining versus substituting designs, improved patellofemoral tracking, and converting flexion-extension gaps. The document outlines the surgical technique for TKA, including approaches, bone cuts, ligament balancing, and the goals of restoring alignment and stability while maximizing range of motion.