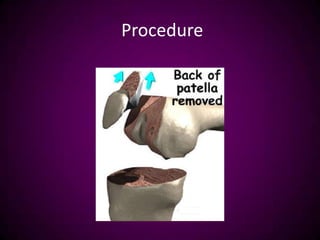
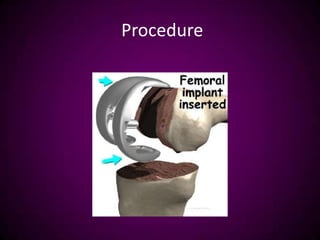
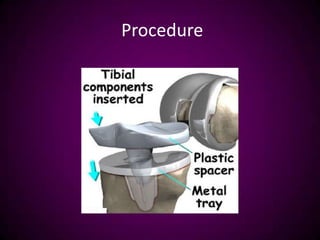
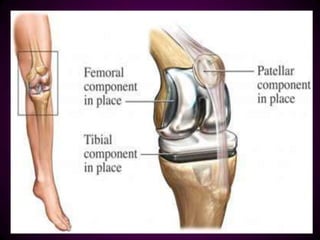
Total knee replacement surgery aims to relieve pain and restore mobility and function. It involves replacing damaged cartilage and bone in the knee joint with prosthetic components. Pre-operative evaluation assesses a patient's medical history, physical exam, labs, and risk factors. Post-operatively, patients undergo physical therapy including range of motion exercises to regain mobility while avoiding high-impact activities. Nursing care focuses on wound monitoring, pain management, and early ambulation to aid recovery.





























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







