Downloaded 366 times














![GIRDLE STONE OSTEOTOMY
In this head & neck of femur are excised at Inter trochanteric
level to create pseudo arthrosis in order to improve stability.
Angulations Osteotomy is added.
INDICATION
• T.B. Hip
• Pyogenic Hip
• Non union #.neck femur [in elderly pt.]
• AVN of femoral head.
Advantage :-
• Painless mobile hip joint](https://image.slidesharecdn.com/osteotomiesaroundthehip-150401110302-conversion-gate01/75/Osteotomies-around-the-hip-25-2048.jpg)













![TRIPLE INNOMINATE OSTEOTOMY BY STEEL
• INDICATIONS- Adolescents &
skeletally mature adults with residual
dysplasia & subluxation in whom
remodelling of acetabulum is no
longer anticipated.
• ADVANTAGE - Better coverage of
femoral head by articular cartilage
[chiari- fibrous cartilage], Better hip
joint stability, no need of spica cast.](https://image.slidesharecdn.com/osteotomiesaroundthehip-150401110302-conversion-gate01/75/Osteotomies-around-the-hip-48-2048.jpg)








































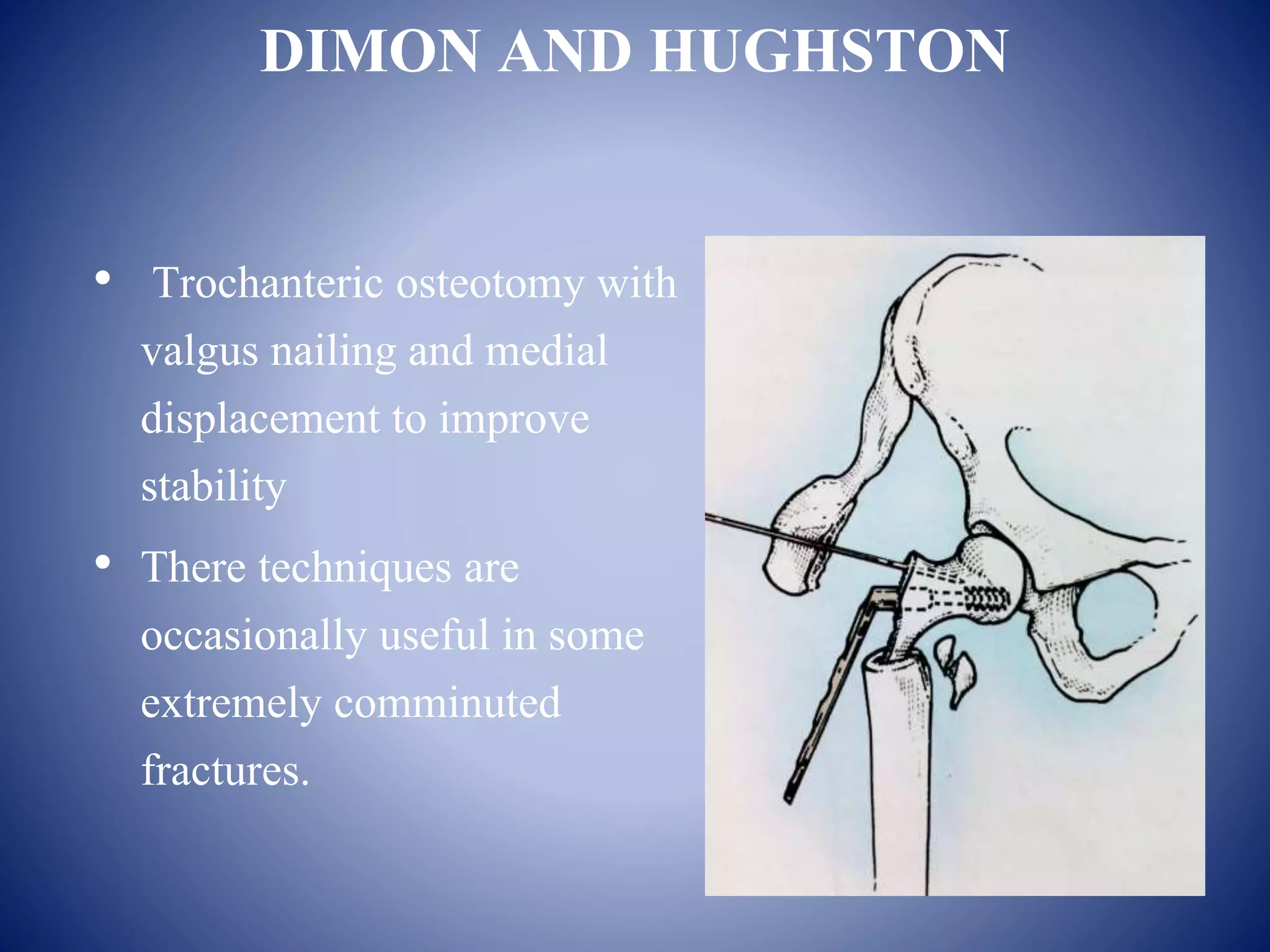
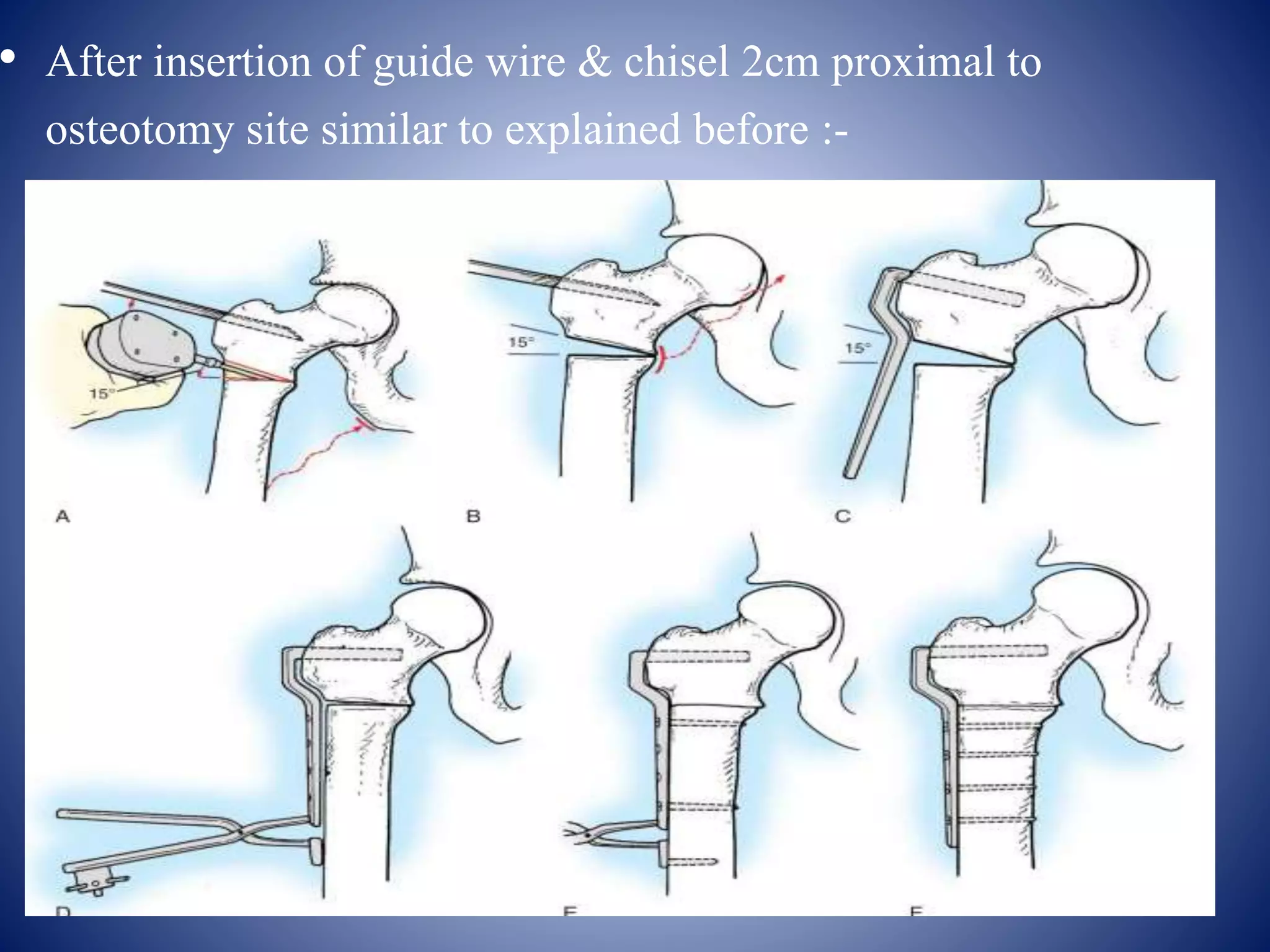
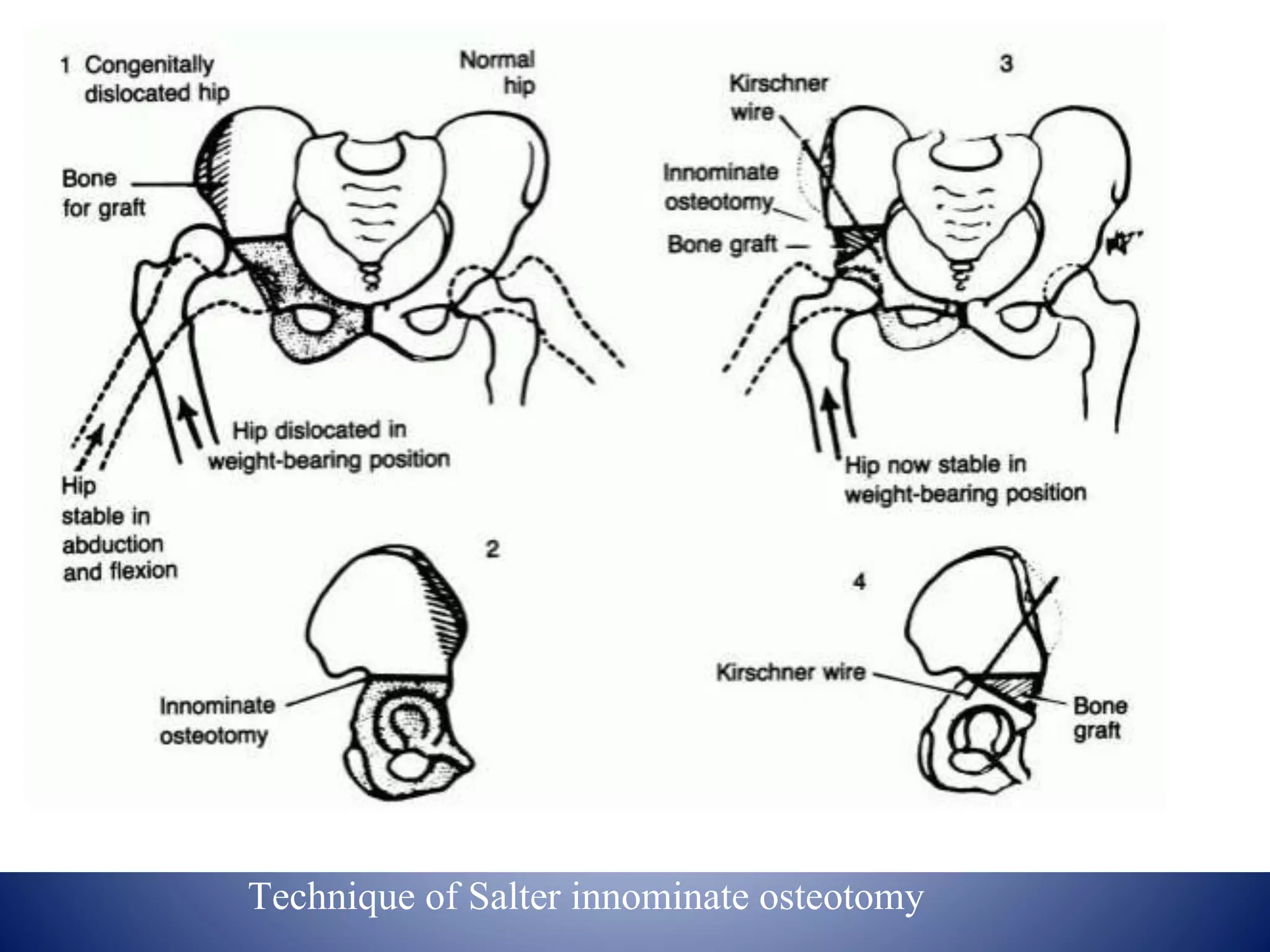
An osteotomy around the hip is a surgical procedure used to correct biomechanical alignment and load transmission. There are various types of osteotomies of the proximal femur classified by displacement of the distal fragment, anatomical location, and indication. Common osteotomies include McMurray's displacement osteotomy, Pauwel's varus/valgus osteotomy, and Salter's innominate osteotomy. The goal of osteotomies is to improve joint congruity, relieve pain, and correct deformities around the hip joint.























































































