Downloaded 185 times
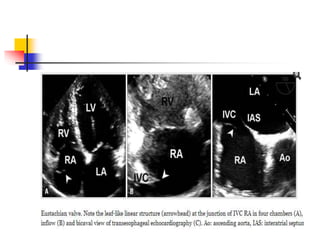
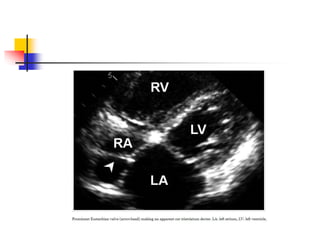
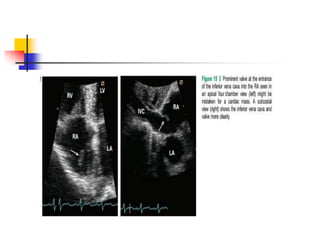
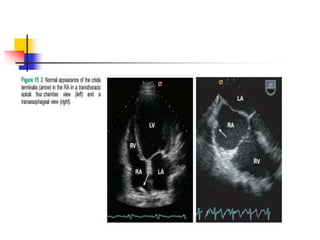
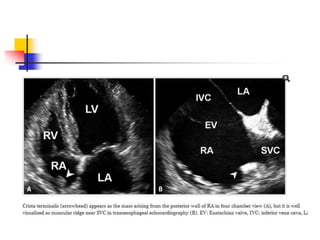
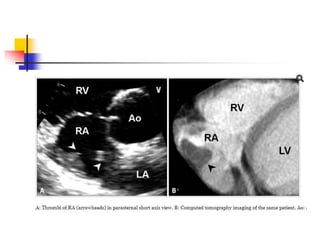


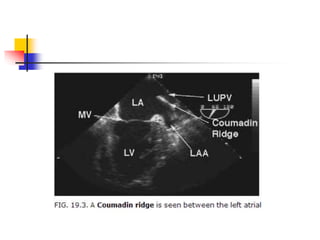
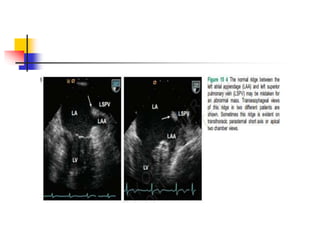



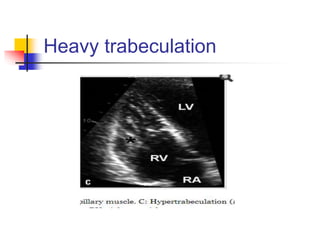
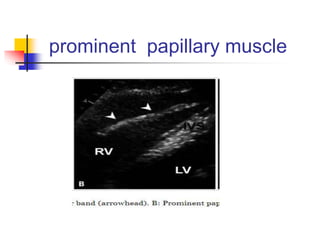
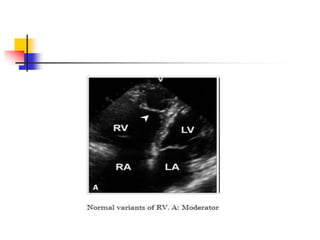
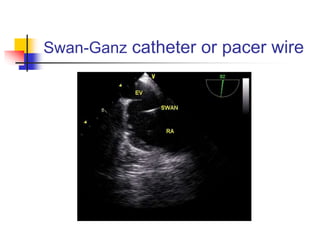


This document discusses several normal anatomic variants that can be mistaken for pathologies in echocardiographic imaging of the heart structures. It describes variants commonly seen in the right atrium, left atrium, left ventricle, aortic valve, and right ventricle which include things like Eustachian valves, Chiari networks, prominent trabeculations, moderator bands, and false tendons. It emphasizes that recognizing these normal variants is important to avoid misdiagnosis and unnecessary treatment based on imaging findings alone.






































































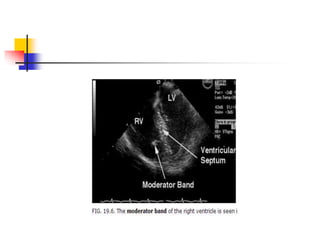
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








